Department of Radiation Oncology, British Columbia Cancer Agency- Vancouver Center, 600 West 10th Avenue, Vancouver, BC, V5Z 4E6, Canada.
Cancer Surveillance and Outcomes, British Columbia Cancer Agency, 703-686 West Broadway, Vancouver, BC, V5Z 4C1, Canada.
Radiat Oncol. 2017 Jun 21;12(1):105. doi: 10.1186/s13014-017-0820-1.
In limited metastatic burden of disease, stereotactic body radiotherapy (SBRT) has been shown to achieve high local control rates. It has been hypothesized that SBRT may translate to a better quality of life by delaying the need for systemic chemotherapy and possibly increasing survival. There is limited published literature on the efficacy of SBRT in limited nodal metastases. The primary aim is to review institutional outcomes of patients with solitary or oligometastatic lymph nodes treated with SBRT.
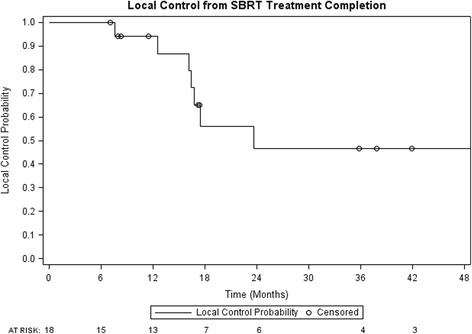
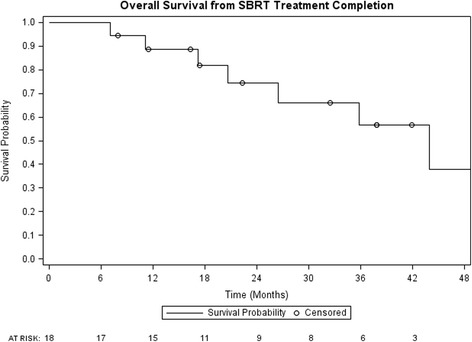
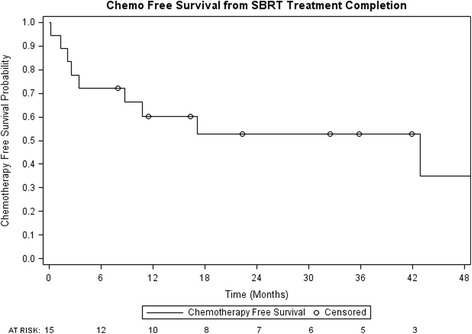
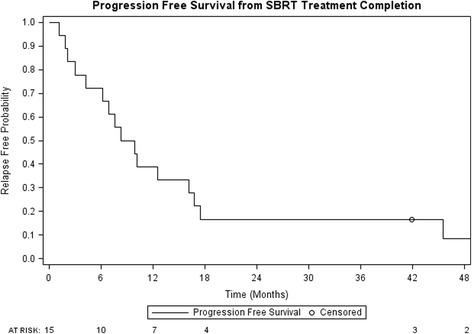
A retrospective study of patients treated with SBRT to metastatic lymph nodes (March 2010-June 2015) was conducted. Endpoints of this study were local control (LC), chemotherapy-free survival (CFS) following SBRT, toxicities, progression free survival (PFS), and overall survival (OS).
Eighteen patients with a mean age of 65 years underwent SBRT to metastatic lymph nodes. Median follow-up was 33.6 months. There were four hepatocellular carcinoma, seven colorectal, four pancreatic, one esophageal, one gallbladder and one lung primary. Eleven (61%) patients had lymph node metastases at initial presentation of metastatic disease. Seven patients (39%) had systemic therapy prior to SBRT, with five patients receiving two lines of chemotherapy. Eight patients had solitary metastatic disease at the time of radiotherapy. All patients had <5 metastases. Median size of lymph node metastases was 1.95 cm (range: 0.8-6.2 cm). RT doses were 31 to 60 Gy in four to ten fractions, with 44% of patients receiving 35 Gy in 5 fractions. At 1 year, LC was 94% and CFS from SBRT was 60%. One-year PFS and OS were 39% and 89% respectively. There were no grade 3 or higher toxicities.
In this single institution study, SBRT to oligometastatic lymph nodes provided excellent LC and a moderate chemotherapy-free interval with minimal toxicities. Disease progression remains prominent in these patients and larger studies are warranted to identify those who benefit most from SBRT.
在疾病转移负担有限的情况下,立体定向体部放疗(SBRT)已被证明能实现高局部控制率。人们假设 SBRT 通过延迟使用全身化疗的需求并可能增加生存时间,从而改善生活质量。关于 SBRT 在局限性淋巴结转移中的疗效,文献报道有限。主要目的是回顾接受 SBRT 治疗的孤立性或寡转移性淋巴结患者的机构治疗结果。
对 2010 年 3 月至 2015 年 6 月期间接受 SBRT 治疗转移性淋巴结的患者进行了回顾性研究。本研究的终点为局部控制(LC)、SBRT 后无化疗生存(CFS)、毒性、无进展生存期(PFS)和总生存期(OS)。
18 名年龄平均为 65 岁的患者接受了 SBRT 治疗转移性淋巴结。中位随访时间为 33.6 个月。原发性肿瘤包括 4 例肝细胞癌、7 例结直肠癌、4 例胰腺癌、1 例食管癌、1 例胆囊癌和 1 例肺癌。11 例(61%)患者在转移性疾病初始表现时即有淋巴结转移。7 例(39%)患者在 SBRT 前接受了全身治疗,其中 5 例接受了 2 线化疗。8 例患者在放疗时仅有孤立性转移病灶。所有患者的转移淋巴结数均<5 个,淋巴结转移灶的中位大小为 1.95cm(范围:0.8-6.2cm)。放疗剂量为 31-60Gy,4-10 次分割,44%的患者接受 35Gy,5 次分割。1 年时,LC 为 94%,SBRT 后的 CFS 为 60%。1 年时的 PFS 和 OS 分别为 39%和 89%。无 3 级或更高毒性。
在本单机构研究中,SBRT 治疗寡转移性淋巴结提供了极好的局部控制率和适度的无化疗间隔期,毒性反应最小。这些患者的疾病进展仍然很明显,需要进行更大规模的研究来确定哪些患者从 SBRT 中获益最多。