Prestwich Andrew, Moore Sally, Kotze Alwyn, Budworth Luke, Lawton Rebecca, Kellar Ian
School of Psychology, University of LeedsLeeds, United Kingdom.
Bradford Institute for Health ResearchBradford, United Kingdom.
Front Psychol. 2017 Jun 7;8:915. doi: 10.3389/fpsyg.2017.00915. eCollection 2017.
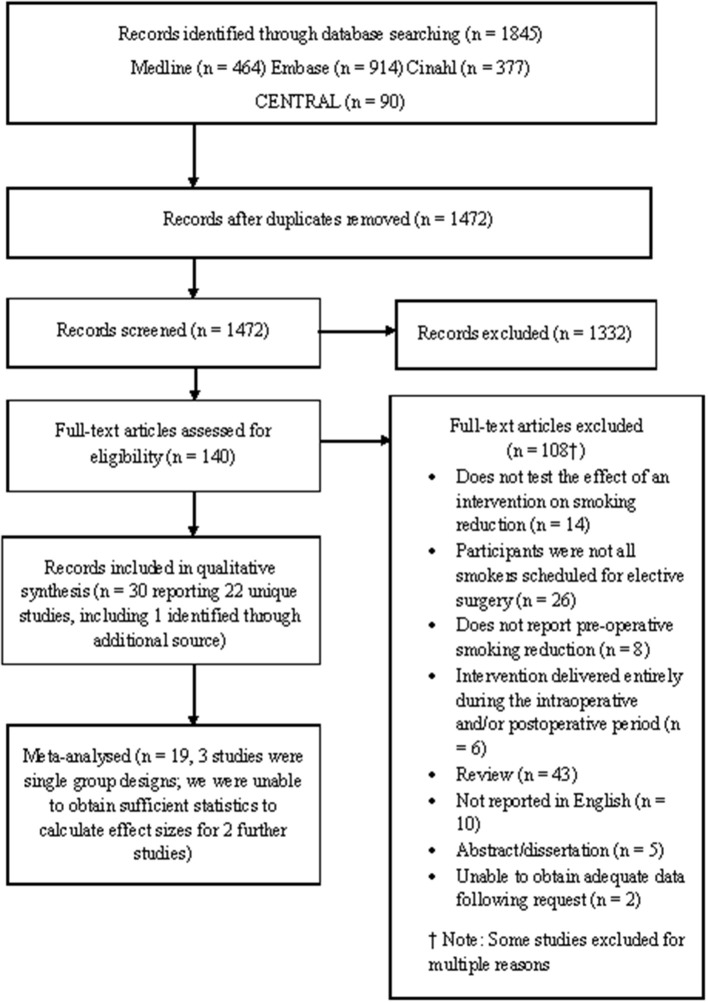
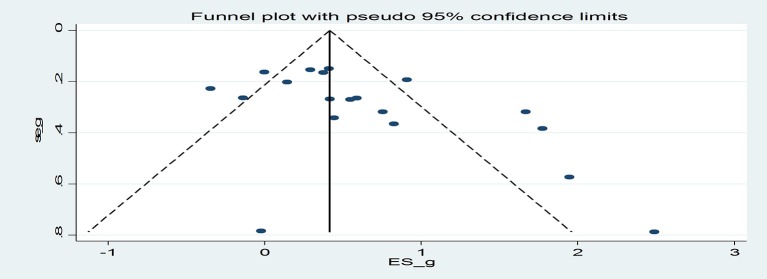
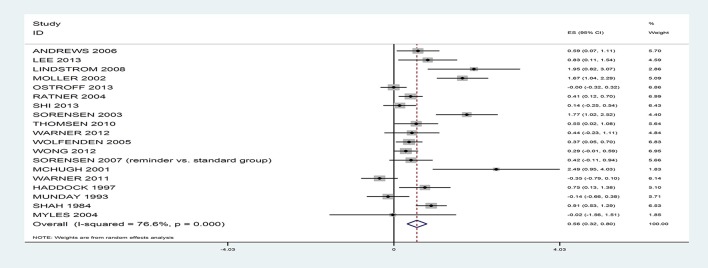
Smokers who continue to smoke up to the point of surgery are at increased risk of a range of complications during and following surgery. To identify whether behavioral and/or pharmacological interventions increase the likelihood that smokers quit prior to elective surgery and which intervention components are associated with larger effects. Systematic review with meta-analysis. MEDLINE, Embase, and Embase Classic, CINAHL, CENTRAL. Studies testing the effect of smoking reduction interventions delivered at least 24 h before elective surgery were included. Potential studies were independently screened by two people. Data relating to study characteristics and risk of bias were extracted. The effects of the interventions on pre-operative smoking abstinence were estimated using random effects meta-analyses. The association between specific intervention components (behavior change techniques; mode; duration; number of sessions; interventionist) and smoking cessation effect sizes were estimated using meta-regressions. Twenty-two studies comprising 2,992 smokers were included and 19 studies were meta-analyzed. Interventions increased the proportion of smokers who were abstinent or reduced smoking by surgery relative to control: = 0.56, 95% CI 0.32-0.80, with rates nearly double in the intervention (46.2%) relative to the control (24.5%). Interventions that comprised more sessions, delivered face-to-face and by nurses, as well as specific behavior change techniques (providing information on consequence of smoking/cessation; providing information on withdrawal symptoms; goal setting; review of goals; regular monitoring by others; and giving options for additional or later support) were associated with larger effects. Rates of smoking can be halved prior to surgery and a number of intervention characteristics can increase these effects. There was, however, some indication of publication bias meaning the benefits of such interventions may be smaller than estimated. Prospero 2015: CRD42015024733.
持续吸烟至手术前的吸烟者在手术期间及术后出现一系列并发症的风险会增加。为了确定行为和/或药物干预是否会增加吸烟者在择期手术前戒烟的可能性,以及哪些干预成分会产生更大的效果。进行系统评价并荟萃分析。检索MEDLINE、Embase、Embase Classic、CINAHL、CENTRAL。纳入了测试在择期手术前至少24小时进行的减少吸烟干预效果的研究。由两人独立筛选潜在研究。提取与研究特征和偏倚风险相关的数据。使用随机效应荟萃分析估计干预对术前戒烟的影响。使用荟萃回归估计特定干预成分(行为改变技术;方式;持续时间;疗程数;干预者)与戒烟效应大小之间的关联。纳入了22项研究,共2992名吸烟者,对其中19项研究进行了荟萃分析。与对照组相比,干预措施增加了在手术时戒烟或减少吸烟的吸烟者比例:RR = 0.56,95%CI 0.32 - 0.80,干预组的比例(46.2%)几乎是对照组(24.5%)的两倍。包括更多疗程、面对面由护士实施以及特定行为改变技术(提供吸烟/戒烟后果信息;提供戒断症状信息;设定目标;目标回顾;他人定期监测;提供额外或后续支持选项)的干预措施效果更大。手术前吸烟率可减半,一些干预特征可增强这些效果。然而,有迹象表明存在发表偏倚,这意味着此类干预的益处可能比估计的要小。Prospero 2015:CRD420