Department of Oncology, Uppsala University Hospital, Uppsala, Sweden.
Department of Surgical Sciences, Radiology, Uppsala University Hospital, Uppsala, Sweden.
J Immunother Cancer. 2017 Jun 20;5:52. doi: 10.1186/s40425-017-0255-0. eCollection 2017.
Accumulating pre-clinical data indicate that the efficient induction of antigen-specific cytotoxic CD8+ T cells characterizing viral infections is caused by cross-priming where initially infected DCs produce an unique set of inflammatory factors that recruit and activate non-infected bystander DCs. Our DC-based immunotherapy concept is guided by such bystander view and accordingly, we have developed a cellular adjuvant consisting of pre-activated allogeneic DCs producing high levels of DC-recruiting and DC-activating factors. This concept doesn't require MHC-compatibility between injected cells and the patient and therefore introduces the possibility of using pre-produced and freeze-stored DCs from healthy blood donors as an off- the-shelf immune enhancer. The use of MHC-incompatible allogeneic DCs will further induce a local rejection process at the injection site that is expected to further enhance recruitment and maturation of endogenous bystander DCs.
Twelve intermediate and poor risk patients with newly diagnosed metastatic renal cell carcinoma (mRCC) where included in a phase I/II study. Pro-inflammatory allogeneic DCs were produced from a leukapheresis product collected from one healthy blood donor and subsequently deep-frozen. A dose of 5-20 × 10 DCs (INTUVAX) was injected into the renal tumor twice with 2 weeks interval before planned nephrectomy and subsequent standard of care.
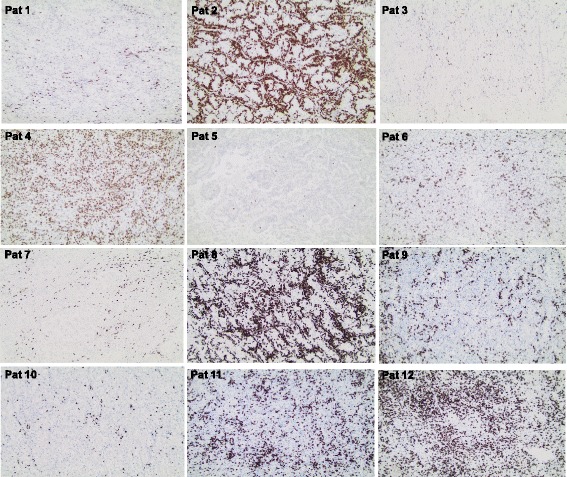
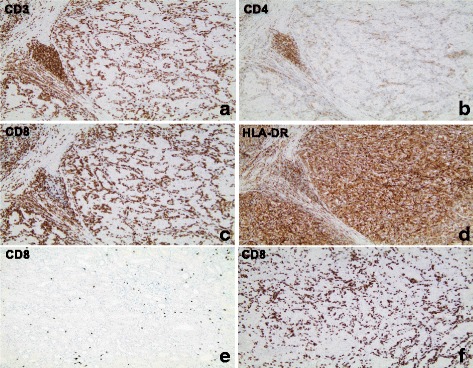
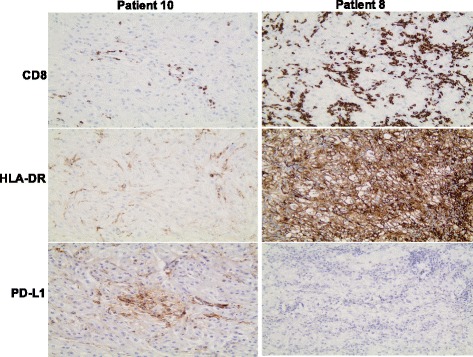
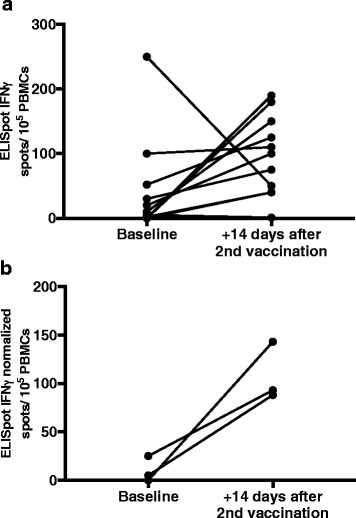
No INTUVAX-related severe adverse events were observed. A massive infiltration of CD8+ T cells was found in 5 out of 12 removed kidney tumors. No objective tumor response was observed and 6 out of 11 evaluable patients have subsequently received additional treatment with standard tyrosine kinase inhibitors (TKI). Three of these 6 patients experienced an objective tumor response including one sunitinib-treated patient who responded with a complete and durable regression of 4 brain metastases. Median overall survival (mOS) is still not reached (currently 42.5 months) but has already passed historical mOS in patients with unfavourable risk mRCC on standard TKI therapy.
Our findings indicate that intratumoral administration of proinflammatory allogeneic DCs induces an anti-tumor immune response that may prolong survival in unfavourable risk mRCC-patients given subsequent standard of care. A randomized, multi-center, phase II mRCC trial (MERECA) with INTUVAX in conjuction with sunitinib has been initiated.
Clinicaltrials.gov identifier: NCT01525017.
越来越多的临床前数据表明,引起病毒感染的抗原特异性细胞毒性 CD8+T 细胞的有效诱导是由交叉引发引起的,最初感染的 DC 产生一组独特的炎症因子,招募并激活未感染的旁观者 DC。我们的基于 DC 的免疫治疗概念是基于这种旁观者观点,因此,我们开发了一种细胞佐剂,由预先激活的同种异体 DC 组成,这些 DC 产生高水平的 DC 招募和激活因子。该概念不需要注射细胞与患者之间的 MHC 相容性,因此引入了使用来自健康献血者的预生产和冷冻储存的 DC 作为现成的免疫增强剂的可能性。使用 MHC 不相容的同种异体 DC 还将在注射部位进一步诱导局部排斥过程,预计这将进一步增强内源性旁观者 DC 的募集和成熟。
12 名新诊断为转移性肾细胞癌(mRCC)的中危和高危患者参与了一项 I/II 期研究。从一名健康献血者采集的白细胞分离物中产生促炎同种异体 DC,随后进行深低温冷冻。在计划进行肾切除术和随后的标准治疗之前,每隔 2 周将 5-20×10 DC(INTUVAX)的剂量注射到肾肿瘤中两次。
未观察到与 INTUVAX 相关的严重不良事件。在 12 个切除的肾脏肿瘤中,有 5 个发现大量 CD8+T 细胞浸润。未观察到客观的肿瘤反应,11 名可评估患者中有 6 名随后接受了标准酪氨酸激酶抑制剂(TKI)的额外治疗。这 6 名患者中的 3 名经历了客观的肿瘤反应,包括 1 名接受舒尼替尼治疗的患者,该患者的 4 个脑转移瘤完全和持久消退。中位总生存期(mOS)仍未达到(目前为 42.5 个月),但已超过标准 TKI 治疗的不良风险 mRCC 患者的历史 mOS。
我们的研究结果表明,同种异体促炎 DC 的肿瘤内给药可诱导抗肿瘤免疫反应,从而延长接受后续标准治疗的不良风险 mRCC 患者的生存时间。已经启动了一项使用 INTUVAX 联合舒尼替尼的肾细胞癌(MERECA)随机、多中心、II 期试验。
Clinicaltrials.gov 标识符:NCT01525017。