Lubbock Alexander L R, Stewart Grant D, O'Mahony Fiach C, Laird Alexander, Mullen Peter, O'Donnell Marie, Powles Thomas, Harrison David J, Overton Ian M
MRC Institute of Genetics and Molecular Medicine, University of Edinburgh, Edinburgh, EH4 2XU, UK.
Present Address: Vanderbilt University School of Medicine, Vanderbilt University, Nashville, Tennessee, USA.
BMC Med. 2017 Jun 26;15(1):118. doi: 10.1186/s12916-017-0874-9.
Metastatic clear cell renal cell cancer (mccRCC) portends a poor prognosis and urgently requires better clinical tools for prognostication as well as for prediction of response to treatment. Considerable investment in molecular risk stratification has sought to overcome the performance ceiling encountered by methods restricted to traditional clinical parameters. However, replication of results has proven challenging, and intratumoural heterogeneity (ITH) may confound attempts at tissue-based stratification.
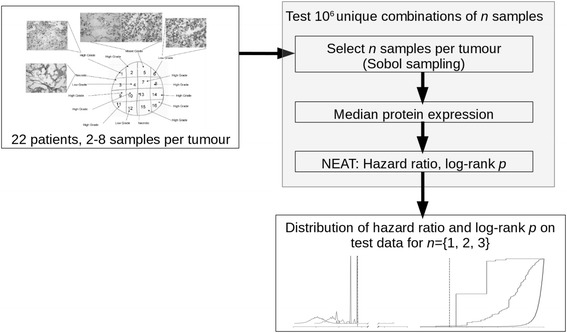
We investigated the influence of confounding ITH on the performance of a novel molecular prognostic model, enabled by pathologist-guided multiregion sampling (n = 183) of geographically separated mccRCC cohorts from the SuMR trial (development, n = 22) and the SCOTRRCC study (validation, n = 22). Tumour protein levels quantified by reverse phase protein array (RPPA) were investigated alongside clinical variables. Regularised wrapper selection identified features for Cox multivariate analysis with overall survival as the primary endpoint.
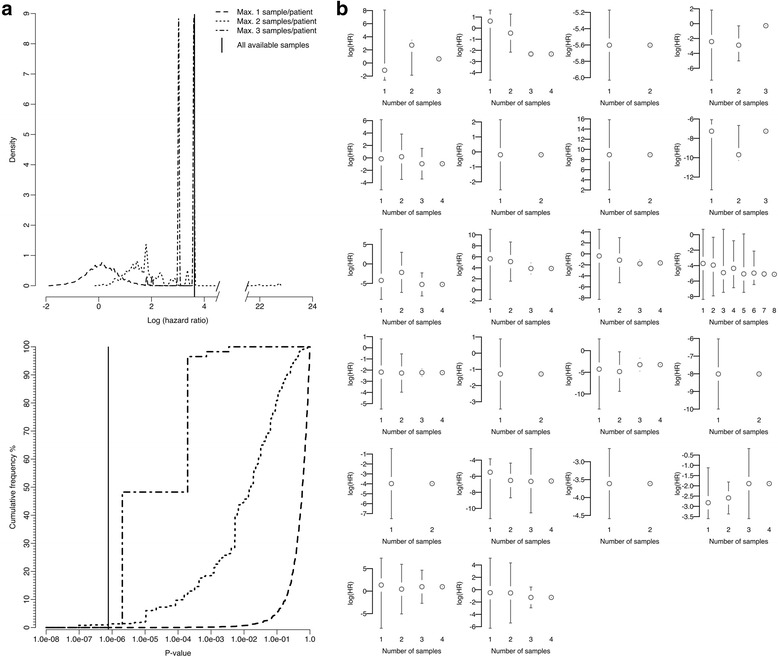
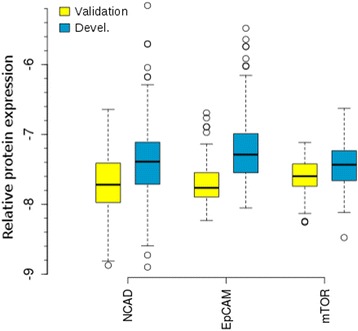
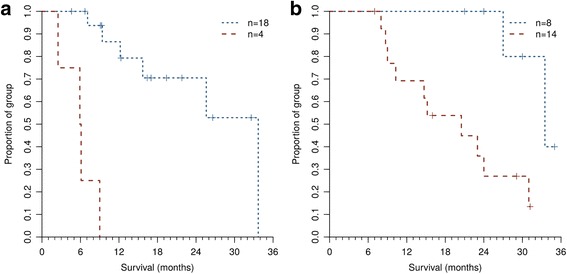
The optimal subset of variables in the final stratification model consisted of N-cadherin, EPCAM, Age, mTOR (NEAT). Risk groups from NEAT had a markedly different prognosis in the validation cohort (log-rank p = 7.62 × 10; hazard ratio (HR) 37.9, 95% confidence interval 4.1-353.8) and 2-year survival rates (accuracy = 82%, Matthews correlation coefficient = 0.62). Comparisons with established clinico-pathological scores suggest favourable performance for NEAT (Net reclassification improvement 7.1% vs International Metastatic Database Consortium score, 25.4% vs Memorial Sloan Kettering Cancer Center score). Limitations include the relatively small cohorts and associated wide confidence intervals on predictive performance. Our multiregion sampling approach enabled investigation of NEAT validation when limiting the number of samples analysed per tumour, which significantly degraded performance. Indeed, sample selection could change risk group assignment for 64% of patients, and prognostication with one sample per patient performed only slightly better than random expectation (median logHR = 0.109). Low grade tissue was associated with 3.5-fold greater variation in predicted risk than high grade (p = 0.044).
This case study in mccRCC quantitatively demonstrates the critical importance of tumour sampling for the success of molecular biomarker studies research where ITH is a factor. The NEAT model shows promise for mccRCC prognostication and warrants follow-up in larger cohorts. Our work evidences actionable parameters to guide sample collection (tumour coverage, size, grade) to inform the development of reproducible molecular risk stratification methods.
转移性透明细胞肾细胞癌(mccRCC)预后较差,迫切需要更好的临床工具用于预后评估以及预测治疗反应。在分子风险分层方面投入了大量精力,试图克服局限于传统临床参数的方法所遇到的性能上限。然而,结果的重复验证颇具挑战,肿瘤内异质性(ITH)可能会干扰基于组织的分层尝试。
我们通过病理学家指导的多区域采样(n = 183),研究了混淆性ITH对一种新型分子预后模型性能的影响,该采样来自SuMR试验(开发组,n = 22)和SCOTRRCC研究(验证组,n = 22)中地理上分离的mccRCC队列。通过反相蛋白阵列(RPPA)定量的肿瘤蛋白水平与临床变量一起进行了研究。正则化包装选择确定了用于以总生存为主要终点的Cox多变量分析的特征。
最终分层模型中的最佳变量子集由N-钙黏蛋白、上皮细胞黏附分子、年龄、雷帕霉素靶蛋白(NEAT)组成。NEAT风险组在验证队列中的预后明显不同(对数秩检验p = 7.62×10;风险比(HR)37.9,95%置信区间4.1 - 353.8),2年生存率(准确性 = 82%,马修斯相关系数 = 0.62)。与既定的临床病理评分比较表明NEAT表现良好(净重新分类改善率与国际转移性数据库联盟评分相比为7.1%,与纪念斯隆凯特琳癌症中心评分相比为25.4%)。局限性包括队列相对较小以及预测性能的相关置信区间较宽。我们的多区域采样方法在限制每个肿瘤分析的样本数量时能够对NEAT进行验证,这显著降低了性能。实际上,样本选择可改变64%患者的风险组分配,每位患者用一个样本进行预后评估仅略优于随机预期(中位对数HR = 0.109)。低级别组织的预测风险变化比高级别组织大3.5倍(p = 0.044)。
该mccRCC案例研究定量证明了肿瘤采样对于ITH是一个因素的分子生物标志物研究成功的至关重要性。NEAT模型在mccRCC预后评估方面显示出前景,值得在更大队列中进行随访。我们的工作证明了可指导样本采集的可行参数(肿瘤覆盖范围、大小、级别),以促进可重复的分子风险分层方法的开发。