Dr. Margarete Fischer-Bosch Institute of Clinical Pharmacology, Auerbachstrasse 112, 70376, Stuttgart, Germany.
University of Tuebingen, Tuebingen, Germany.
BMC Med. 2018 Jul 5;16(1):108. doi: 10.1186/s12916-018-1088-5.
Stratification of cancer patients to identify those with worse prognosis is increasingly important. Through in silico analyses, we recently developed a gene expression-based prognostic score (S3-score) for clear cell renal cell carcinoma (ccRCC), using the cell type-specific expression of 97 genes within the human nephron. Herein, we verified the score using whole-transcriptome data of independent cohorts and extend its application for patients with metastatic disease receiving tyrosine kinase inhibitor treatment. Finally, we sought to improve the signature for clinical application using qRT-PCR.
A 97 gene-based S3-score (S3) was evaluated in a set of 52 primary non-metastatic and metastatic ccRCC patients as well as in 53 primary metastatic tumors of sunitinib-treated patients. Gene expression data of The Cancer Genome Atlas (n = 463) was used for platform transfer and development of a simplified qRT-PCR-based 15-gene S3-score (S3). This S3-score was validated in 108 metastatic and non-metastatic ccRCC patients and ccRCC-derived metastases including in part several regions from one metastasis. Univariate and multivariate Cox regression stratified by T, N, M, and G were performed with cancer-specific and progression-free survival as primary endpoints.
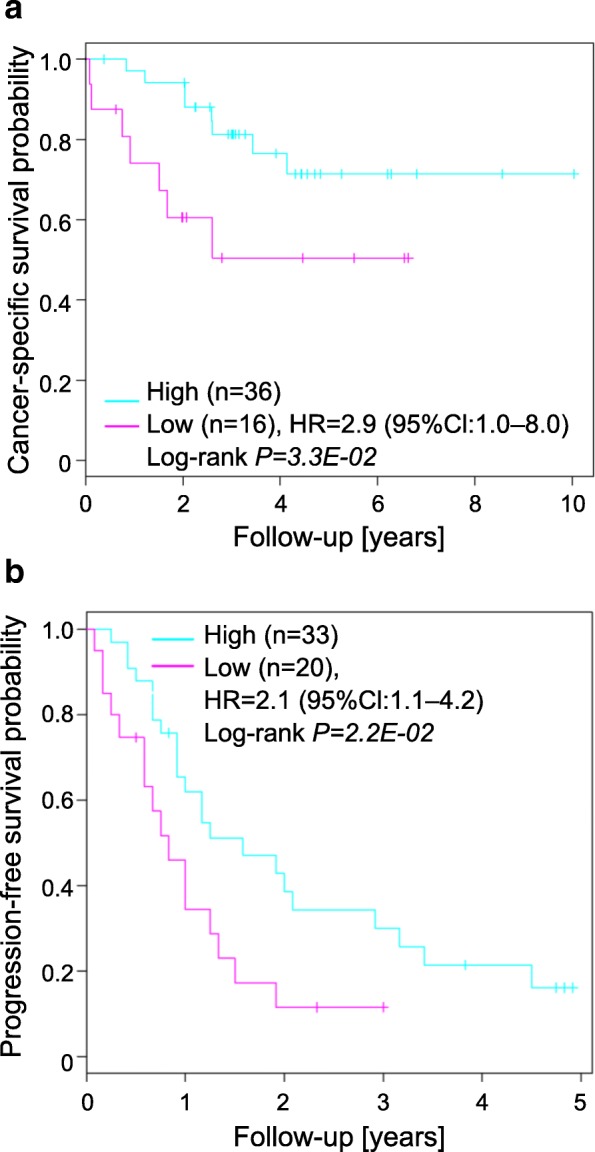
The S3-score was significantly associated with cancer-specific survival (CSS) in 52 ccRCC patients (HR 2.9, 95% Cl 1.0-8.0, P = 3.3 × 10) as well as progression-free survival in sunitinib-treated patients (2.1, 1.1-4.2, P = 2.2 × 10). The qRT-PCR based S3-score performed similarly to the S3-score, and was significantly associated with CSS in our extended cohort of 108 patients (5.0, 2.1-11.7, P = 5.1 × 10) including metastatic (9.3, 1.8-50.0, P = 2.3 × 10) and non-metastatic patients (4.4, 1.2-16.3, P = 1.6 × 10), even in multivariate Cox regression, including clinicopathological parameters (7.3, 2.5-21.5, P = 3.3 × 10). Matched primary tumors and metastases revealed similar S3-scores, thus allowing prediction of outcome from metastatic tissue. The molecular-based qRT-PCR S3-score significantly improved prediction of CSS by the established clinicopathological-based SSIGN score (P = 1.6 × 10).
The S3-score offers a new clinical avenue for ccRCC risk stratification in the non-metastatic, metastatic, and sunitinib-treated setting.
对癌症患者进行分层以识别预后较差的患者变得越来越重要。通过计算机模拟分析,我们最近使用人类肾单位中 97 种基因的细胞类型特异性表达,为透明细胞肾细胞癌(ccRCC)开发了一种基于基因表达的预后评分(S3 评分)。在此,我们使用独立队列的全转录组数据验证了该评分,并将其应用扩展到接受酪氨酸激酶抑制剂治疗的转移性疾病患者。最后,我们试图使用 qRT-PCR 来改进该特征以用于临床应用。
在一组 52 例原发性非转移性和转移性 ccRCC 患者以及 53 例接受舒尼替尼治疗的转移性肿瘤患者中评估了基于 97 个基因的 S3 评分(S3)。使用癌症基因组图谱(n=463)的数据进行平台转移,并开发了简化的基于 qRT-PCR 的 15 基因 S3 评分(S3)。该 S3 评分在 108 例转移性和非转移性 ccRCC 患者以及包括部分来自一个转移灶的多个区域的 ccRCC 转移灶中进行了验证。使用癌症特异性和无进展生存期作为主要终点,对 T、N、M 和 G 进行单变量和多变量 Cox 回归分层。
S3 评分与 52 例 ccRCC 患者的癌症特异性生存期(CSS)显著相关(HR 2.9,95%Cl 1.0-8.0,P=3.3×10),与舒尼替尼治疗患者的无进展生存期也显著相关(2.1,1.1-4.2,P=2.2×10)。基于 qRT-PCR 的 S3 评分与 S3 评分表现相似,与我们扩展的 108 例患者队列的 CSS 显著相关(5.0,2.1-11.7,P=5.1×10),包括转移性(9.3,1.8-50.0,P=2.3×10)和非转移性患者(4.4,1.2-16.3,P=1.6×10),甚至在包括临床病理参数的多变量 Cox 回归中也是如此(7.3,2.5-21.5,P=3.3×10)。匹配的原发性肿瘤和转移灶显示出相似的 S3 评分,因此可以从转移性组织预测结果。基于分子的 qRT-PCR S3 评分通过既定的临床病理 SSIGN 评分显著提高了 CSS 的预测能力(P=1.6×10)。
S3 评分在非转移性、转移性和接受舒尼替尼治疗的环境中为 ccRCC 风险分层提供了新的临床途径。