Froedtert and the Medical College of Wisconsin, Milwaukee, Wisconsin.
NRG Oncology Statistics and Data Management Center, Philadelphia, Pennsylvania; Johns Hopkins University, Baltimore, Maryland.
J Thorac Oncol. 2017 Oct;12(10):1561-1570. doi: 10.1016/j.jtho.2017.06.015. Epub 2017 Jun 23.
NRG Oncology RTOG 0937 is a randomized phase II trial evaluating 1-year overall survival (OS) with prophylactic cranial irradiation (PCI) or PCI plus consolidative radiation therapy (PCI+cRT) to intrathoracic disease and extracranial metastases for extensive-disease SCLC.
Patients with one to four extracranial metastases were eligible after a complete response or partial response to chemotherapy. Randomization was to PCI or PCI+cRT to the thorax and metastases. Original stratification included partial response versus complete response after chemotherapy and one versus two to four metastases; age younger than 65 years versus 65 years or older was added after an observed imbalance. PCI consisted of 25 Gy in 10 fractions. cRT consisted of 45 Gy in 15 fractions. To detect an improvement in OS from 30% to 45% with a 34% hazard reduction (hazard ratio = 0.66) under a 0.1 type 1 error (one sided) and 80% power, 154 patients were required.
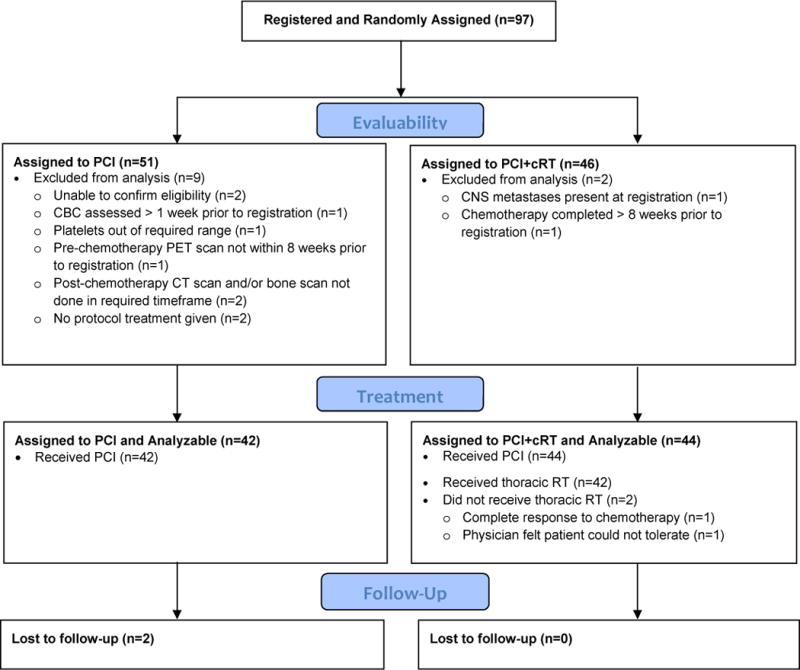
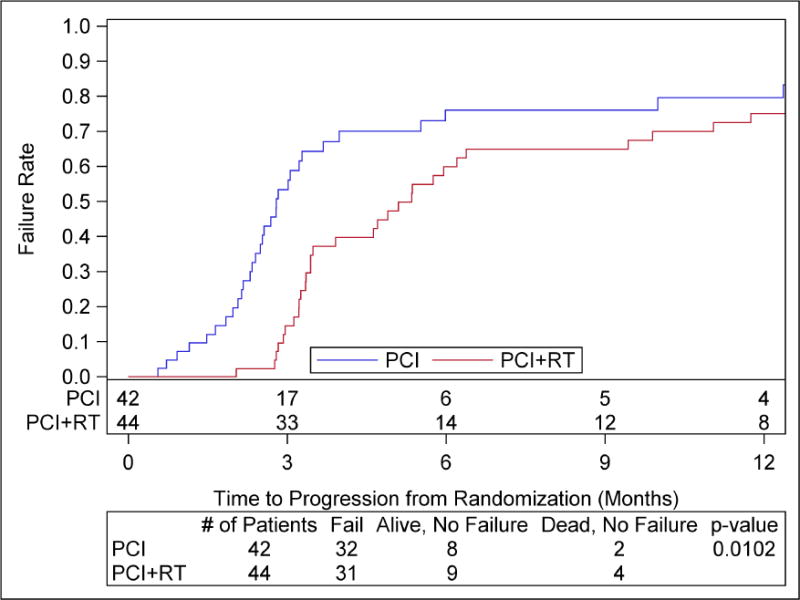
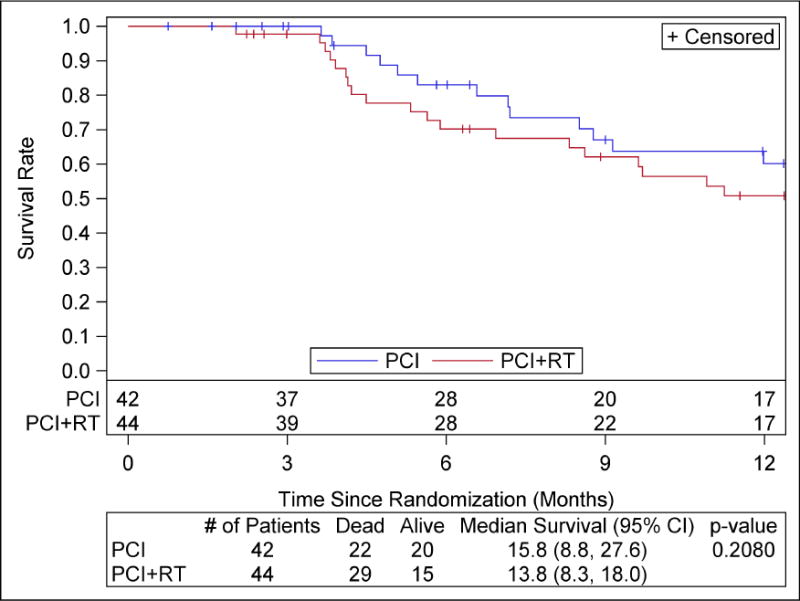
A total of 97 patients were randomized between March 2010 and February 2015. Eleven patients were ineligible (nine in the PCI group and two in the PCI+cRT group), leaving 42 randomized to receive PCI and 44 to receive PCI+cRT. At planned interim analysis, the study crossed the futility boundary for OS and was closed before meeting the accrual target. Median follow-up was 9 months. The 1-year OS was not different between the groups: 60.1% (95% confidence interval [CI]: 41.2-74.7) for PCI and 50.8% (95% CI: 34.0-65.3) for PCI+cRT (p = 0.21). The 3- and 12-month rates of progression were 53.3% and 79.6% for PCI and 14.5% and 75% for PCI+cRT, respectively. Time to progression favored PCI+cRT (hazard ratio = 0.53, 95% CI: 0.32-0.87, p = 0.01). One patient in each arm had grade 4 therapy-related toxicity and one had grade 5 therapy-related pneumonitis with PCI+cRT.
OS exceeded predictions for both arms. cRT delayed progression but did not improve 1-year OS.
NRG Oncology RTOG 0937 是一项随机的二期临床试验,评估了预防性颅脑照射(PCI)或 PCI 联合巩固性放疗(PCI+cRT)对广泛期小细胞肺癌(SCLC)的胸内疾病和颅外转移的 1 年总生存期(OS)。
在化疗完全缓解或部分缓解后,有 1 至 4 个颅外转移的患者符合条件。患者被随机分配至 PCI 或 PCI+cRT 治疗胸部和转移灶。原始分层包括化疗后部分缓解与完全缓解,1 至 4 个转移灶;65 岁以下与 65 岁或以上年龄。观察到不平衡后,加入年龄小于 65 岁与年龄大于等于 65 岁。PCI 组包括 25 Gy 的 10 次分割。cRT 组包括 45 Gy 的 15 次分割。为了在 30%的 OS 基础上提高到 45%,并在 0.1 的单侧Ⅰ类错误(type 1 error)和 80%的功效下,需要 154 例患者。
2010 年 3 月至 2015 年 2 月期间共随机分配了 97 例患者。11 例患者不符合条件(9 例在 PCI 组,2 例在 PCI+cRT 组),42 例随机接受 PCI 治疗,44 例接受 PCI+cRT 治疗。在计划的中期分析中,该研究的 OS 达到了无效性边界,在达到入组目标之前就已关闭。中位随访时间为 9 个月。两组 1 年 OS 无差异:PCI 组为 60.1%(95%CI:41.2-74.7),PCI+cRT 组为 50.8%(95%CI:34.0-65.3)(p=0.21)。PCI 组的 3 个月和 12 个月的进展率分别为 53.3%和 79.6%,PCI+cRT 组分别为 14.5%和 75%。进展时间有利于 PCI+cRT(危险比为 0.53,95%CI:0.32-0.87,p=0.01)。每组各有 1 例患者发生 4 级治疗相关毒性,1 例患者发生 5 级治疗相关肺炎,与 PCI+cRT 相关。
两组 OS 均高于预测值。cRT 延缓了进展,但未改善 1 年 OS。