Nakamura Takashi, Nakamura Akihisa, Mukuda Kengo, Harada Masanori, Kotani Kazuhiko
Center for Community Medicine, Jichi Medical University, 3311-1 Yakushiji Shimotsuke, Tochigi, 3290498, Japan.
Gero Municipal Osaka Clinic, 1965 Ohshima Osaka Gero, Gifu, 5093106, Japan.
BMC Health Serv Res. 2017 Jun 26;17(1):438. doi: 10.1186/s12913-017-2367-0.
For achieving equity of the accessibility to primary healthcare, measuring potential geographical accessibility is essential. The provider-to-population ratio is the most frequently used measure. However, it is difficult to be used in closer region because it does not take into consideration the people and health services beyond its boundary. In order to overcome this problem, we measured the potential access to hospital, using both distance measures and the enhanced two-step floating catchment area (E2SFCA) method. The aim of this study was to compare the number of hospitals in the neighborhood and the E2SFCA score with regard to the amount and equity for access to hospitals.
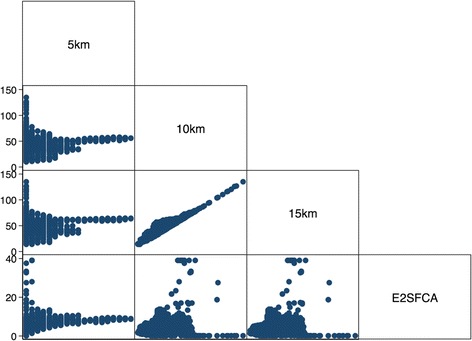
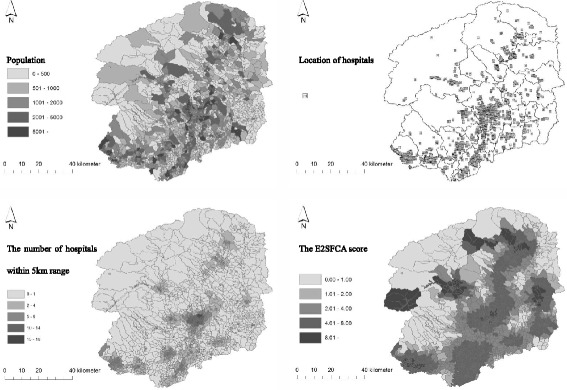
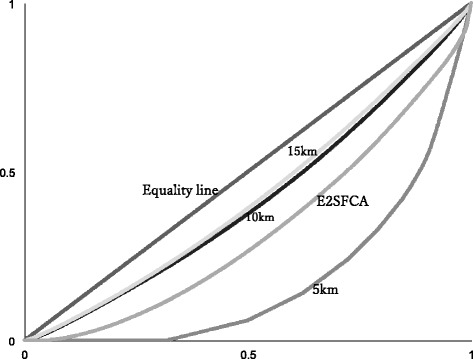
This descriptive study used publicly available data from 2010. The E2SFCA score and number of neighborhood hospitals were obtained from Tochigi province in Japan using a geographic information system. Dataset of four measures by each census tract was obtained. The measures were E2SFCA score, number of hospitals within the 5 km range, number of hospitals within the 10 km range, and number of hospitals within the 15 km range. Correlation and disparity analyses with the Lorenz curve and Gini coefficient were performed.
The measures were obtained in a smaller area than municipality considering adjacent areas using a geographical approach. The E2SFCA score was 5.3 [3.2-7.3] hospitals/million (median [quantile range]), compared to 5.6 hospitals/million in total for the given district. The median number of hospitals within the 5 km, 10 km, and 15 km ranges were 1, 39, and 47, respectively. There was no hospital within the 5 km range in one third of the blocks. Both the number of hospitals within the 10 km range and those within the 15 km range were well correlated. Regional difference became smaller as the distance to count the number of hospitals increased. The gap between small number of hospitals and the high E2SFCA score indicated the location of community hospital in depopulated areas.
The E2SFCA method is superior for analyzing spatial access to hospital, because it provides information in the closer sub-regions. Regional differences were hardly seen in access to hospital beyond the 10 km range. Further studies in other regions and countries are needed for precise assessment.
为实现初级医疗保健可及性的公平性,衡量潜在的地理可及性至关重要。医疗服务提供者与人口的比例是最常用的衡量指标。然而,由于它没有考虑其边界之外的人口和医疗服务,因此在较小区域内难以使用。为了克服这个问题,我们使用距离测量法和改进的两步浮动捕获区域(E2SFCA)方法来衡量医院的潜在可及性。本研究的目的是比较邻里医院数量和E2SFCA得分在医院可及性的数量和公平性方面的情况。
这项描述性研究使用了2010年的公开可用数据。通过地理信息系统从日本枥木县获取E2SFCA得分和邻里医院数量。获得了每个普查区的四项测量数据集。这些测量指标为E2SFCA得分、5公里范围内的医院数量、10公里范围内的医院数量以及15公里范围内的医院数量。使用洛伦兹曲线和基尼系数进行相关性和差异分析。
与考虑相邻区域的市政区域相比,这些测量是在更小的区域内进行的。E2SFCA得分为5.3[3.2 - 7.3]家医院/百万(中位数[分位数范围]),而给定区域的总数为5.6家医院/百万。5公里、10公里和15公里范围内医院数量的中位数分别为1、39和47。三分之一的街区在5公里范围内没有医院。10公里范围内的医院数量和15公里范围内的医院数量相关性良好。随着计算医院数量的距离增加,区域差异变小。医院数量少与E2SFCA得分高之间的差距表明社区医院位于人口稀少地区。
E2SFCA方法在分析医院的空间可及性方面更具优势,因为它能在更接近的子区域提供信息。在10公里范围之外,医院可及性方面几乎没有区域差异。需要在其他地区和国家进行进一步研究以进行精确评估。