Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Parkland Health and Hospital System, Dallas, Texas, USA.
BMJ Qual Saf. 2017 Oct;26(10):832-836. doi: 10.1136/bmjqs-2017-006671. Epub 2017 Jun 26.
Respiratory rate (RR) is an independent predictor of adverse outcomes and an integral component of many risk prediction scores for hospitalised adults. Yet, it is unclear if RR is recorded accurately. We sought to assess the potential accuracy of RR by analysing the distribution and variation as a proxy, since RR should be normally distributed if recorded accurately.
We conducted a descriptive observational study of electronic health record data from consecutive hospitalisations from 2009 to 2010 from six diverse hospitals. We assessed the distribution of the maximum RR on admission, using heart rate (HR) as a comparison since this is objectively measured. We assessed RR patterns among selected subgroups expected to have greater physiological variation using the coefficient of variation (CV=SD/mean).
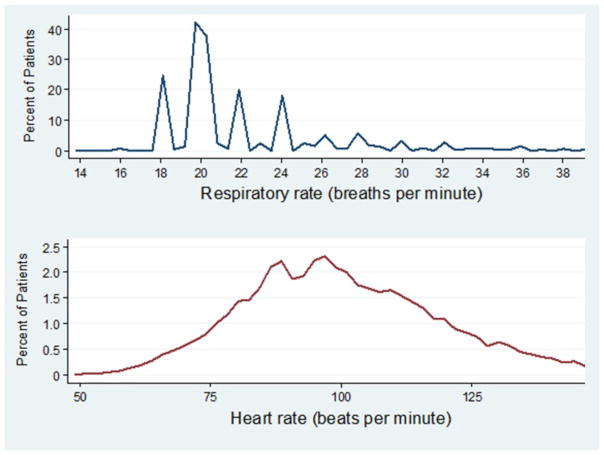
Among 36 966 hospitalisations, recorded RR was not normally distributed (p<0.001), but right skewed (skewness=3.99) with values clustered at 18 and 20 (kurtosis=23.9). In contrast, HR was relatively normally distributed. Patients with a cardiopulmonary diagnosis or hypoxia only had modestly greater variation (CV increase of 2%-6%). Among 1318 patients transferred from the ward to the intensive care unit (n=1318), RR variation the day preceding transfer was similar to that observed on admission (CV 0.24 vs 0.26), even for those transferred with respiratory failure (CV 0.25).
The observed patterns suggest that RR is inaccurately recorded, even among those with cardiopulmonary compromise, and represents a 'spot' estimate with values of 18 and 20 breaths per minute representing 'normal.' While spot estimates may potentially be adequate to indicate clinical stability, inaccurate RR may alternatively lead to misclassification of disease severity, potentially jeopardising patient safety. Thus, we recommend greater training for hospital personnel to accurately record RR.
呼吸频率(RR)是不良预后的独立预测因子,也是许多住院成人风险预测评分的组成部分。然而,RR 是否准确记录尚不清楚。我们试图通过分析分布和变异性来评估 RR 的潜在准确性,因为如果 RR 准确记录,它应该是正态分布的。
我们对来自六家不同医院的 2009 年至 2010 年连续住院患者的电子健康记录数据进行了描述性观察研究。我们评估了入院时最大 RR 的分布,将心率(HR)作为比较,因为这是客观测量的。我们使用变异系数(CV=SD/mean)评估了预期生理变化较大的选定亚组的 RR 模式。
在 36966 例住院患者中,记录的 RR 分布不正态(p<0.001),但右偏(偏度=3.99),值集中在 18 和 20(峰度=23.9)。相比之下,HR 相对正态分布。有心肺诊断或仅缺氧的患者变化幅度略大(CV 增加 2%-6%)。在从病房转至重症监护病房的 1318 例患者中(n=1318),转院前一天的 RR 变化与入院时观察到的变化相似(CV 0.24 与 0.26),即使是呼吸衰竭患者(CV 0.25)。
观察到的模式表明,RR 记录不准确,即使在心肺功能受损的患者中也是如此,并且代表每分钟 18 和 20 次呼吸的“单点”估计值表示“正常”。虽然单点估计值可能足以表明临床稳定,但 RR 不准确可能会导致疾病严重程度的错误分类,从而危及患者安全。因此,我们建议对医院人员进行更多的 RR 记录培训。