Bernasconi Maurizio, Koegelenberg Coenraad F N, Koutsokera Angela, Ogna Adam, Casutt Alessio, Nicod Laurent, Lovis Alban
Division of Pulmonology, Dept of Medicine, University Hospital of Lausanne, Lausanne, Switzerland.
Division of Pulmonology, Dept of Medicine, Stellenbosch University and Tygerberg Academic Hospital, Cape Town, South Africa.
ERJ Open Res. 2017 Jun 21;3(2). doi: 10.1183/23120541.00084-2016. eCollection 2017 Apr.
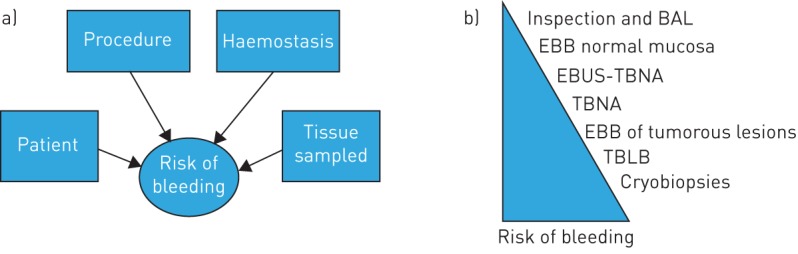
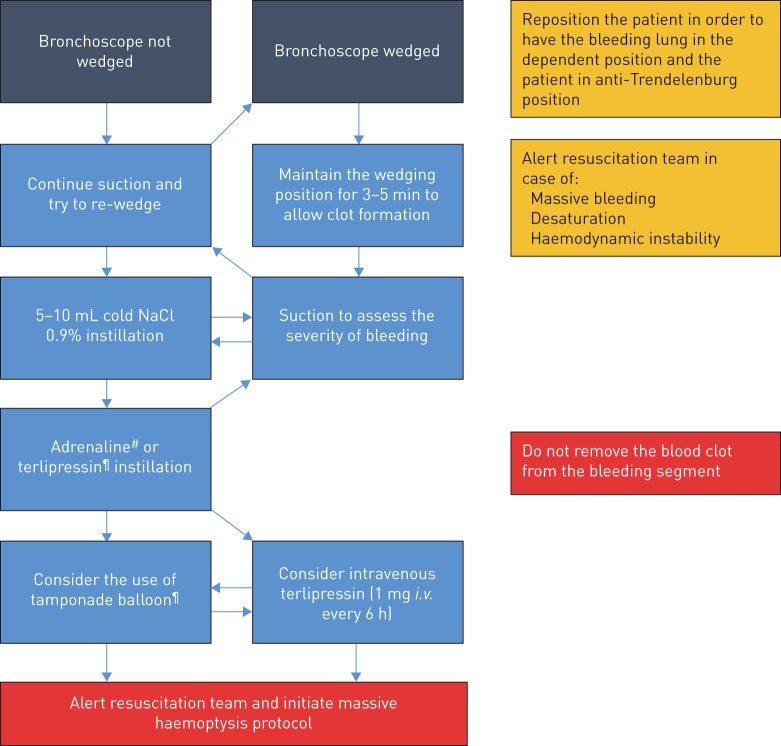
Significant iatrogenic bleeding during flexible bronchoscopy is fortunately rare and usually self-limiting. Life-threatening bleeding, however, can occur, especially after conventional or cryoprobe-assisted transbronchial biopsy. The aim of this review is to provide the practising pulmonologist with a concise overview of the incidence, severity and risk factors for bleeding, to provide sensible advice on prophylactic measures and to suggest a plan of action in the case of significant bleeding. Bronchoscopy units should have a standardised approach and plan of action in the case of life-threatening haemorrhage. Wedging the bronchoscope in the bleeding segment, turning the patient in an anti-Trendelenburg position and onto the side in order for the bleeding lung to be in the dependent position, installing vasoconstrictors and using a tamponade balloon early are the recommended first-line strategies. Involving a resuscitation team should be considered early in the case of massive bleeding, desaturation and haemodynamic instability.
幸运的是,在柔性支气管镜检查期间发生的严重医源性出血很少见,且通常为自限性。然而,危及生命的出血可能会发生,尤其是在传统或冷冻探头辅助经支气管活检后。本综述的目的是为执业肺科医生提供关于出血的发生率、严重程度和危险因素的简要概述,提供关于预防措施的合理建议,并提出在发生严重出血时的行动计划。支气管镜检查科室在面对危及生命的出血情况时应采用标准化的方法和行动计划。将支气管镜楔入出血段、将患者置于反特伦德伦伯格体位并侧卧以使出血侧肺处于下垂位置、早期安装血管收缩剂并使用填塞球囊是推荐的一线策略。在发生大量出血、低氧血症和血流动力学不稳定的情况下,应尽早考虑召集复苏团队。