Department of Cardiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Department of Epidemiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Cardiovasc Drugs Ther. 2017 Jun;31(3):281-293. doi: 10.1007/s10557-017-6726-1.
Over the last 50 years, clinical trials of novel interventions for acute heart failure (AHF) have, with few exceptions, been neutral or shown harm. We hypothesize that this might be related to a differential response to pharmacological therapy.
We studied the magnitude of treatment effect of rolofylline across clinical characteristics and plasma biomarkers in 2033 AHF patients and derived a biomarker-based responder sum score model. Treatment response was survival from all-cause mortality through day 180.
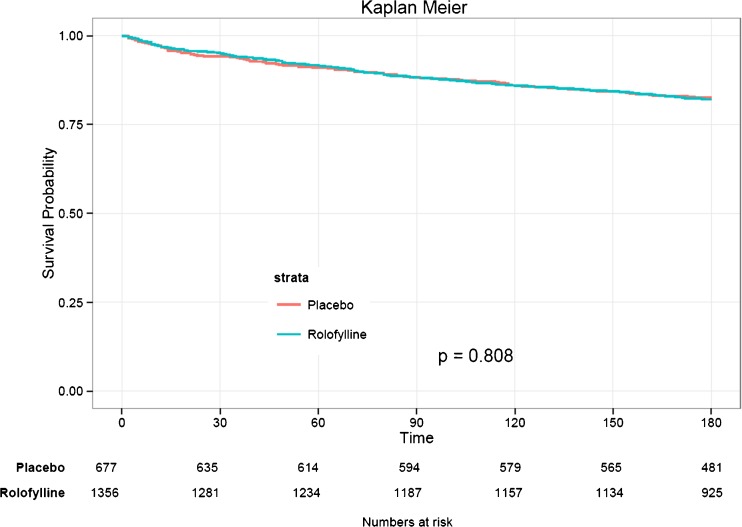
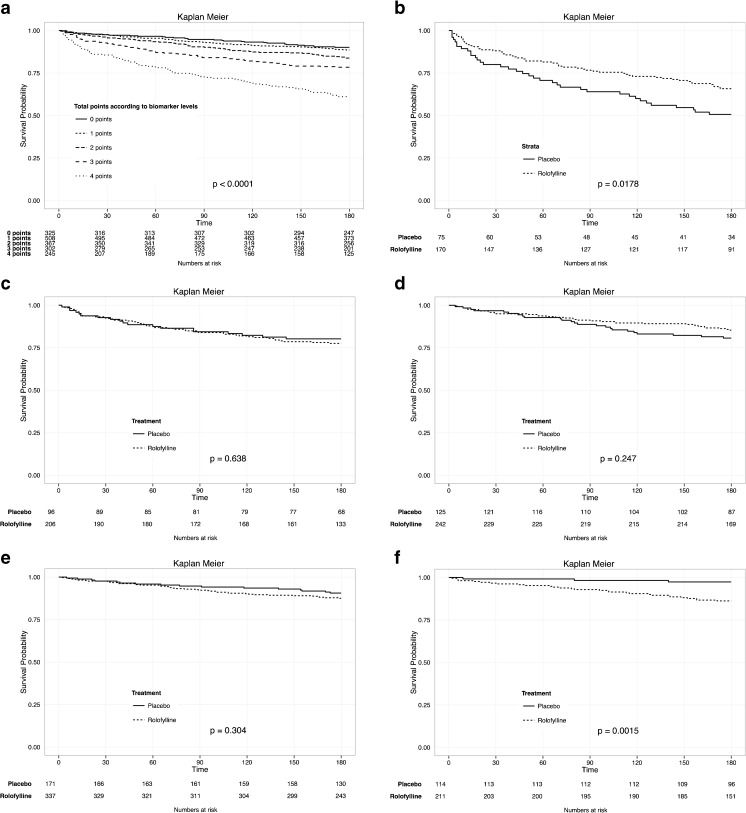
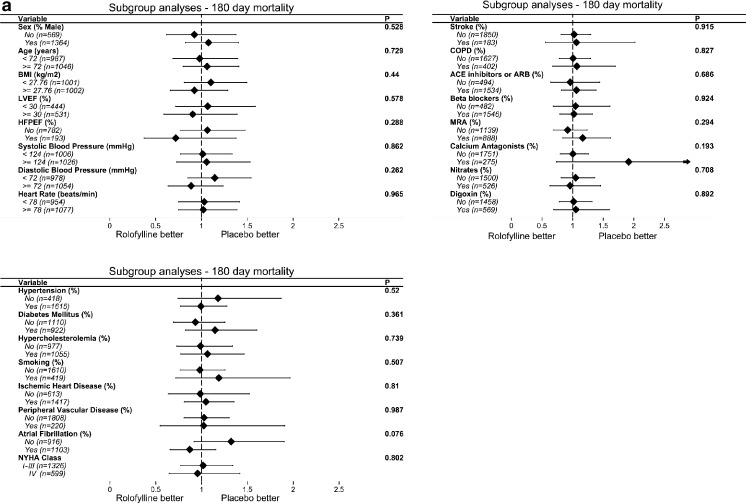
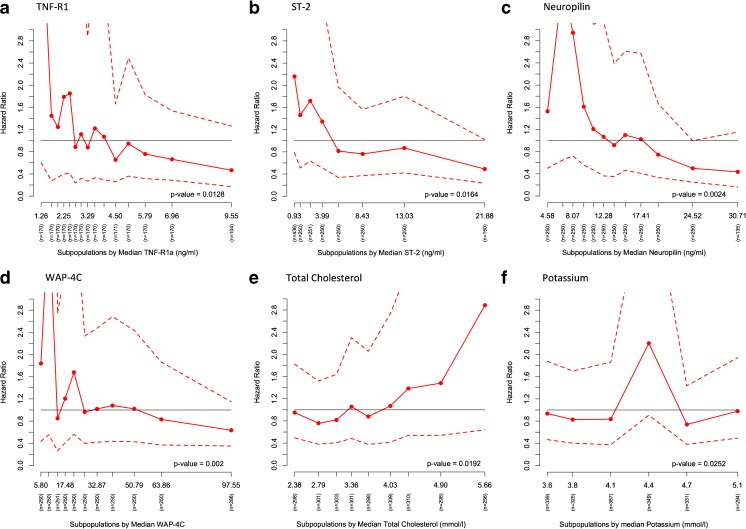
In the overall study population, rolofylline had no effect on mortality (HR 1.03, 95% CI 0.82-1.28, p = 0.808). We found no treatment interaction across clinical characteristics, but we found interactions between several biomarkers and rolofylline. The biomarker-based sum score model included TNF-R1α, ST2, WAP four-disulfide core domain protein HE4 (WAP-4C), and total cholesterol, and the score ranged between 0 and 4. In patients with score 4 (those with increased TNF-R1α, ST2, WAP-4C, and low total cholesterol), treatment with rolofylline was beneficial (HR 0.61, 95% CI 0.40-0.92, p = 0.019). In patients with score 0, treatment with rolofylline was harmful (HR 5.52, 95% CI 1.68-18.13, p = 0.005; treatment by score interaction p < 0.001). Internal validation estimated similar hazard ratio estimates (0 points: HR 5.56, 95% CI 5.27-7-5.87; 1 point: HR 1.31, 95% CI 1.25-1.33; 2 points: HR 0.75, 95% CI 0.74-0.76; 3 points: HR 1.13, 95% CI 1.11-1.15; 4 points, HR 0.61, 95% CI 0.61-0.62) compared to the original data.
Biomarkers are superior to clinical characteristics to study treatment heterogeneity in acute heart failure.
在过去的 50 年中,急性心力衰竭(AHF)新型干预措施的临床试验,除了少数例外,结果均为中性或显示有害。我们假设这可能与对药物治疗的不同反应有关。
我们研究了罗氟司特在 2033 例 AHF 患者的临床特征和血浆生物标志物中的治疗效果,并得出了基于生物标志物的应答者总和评分模型。治疗反应是通过第 180 天的全因死亡率的生存情况。
在整个研究人群中,罗氟司特对死亡率没有影响(HR 1.03,95%CI 0.82-1.28,p=0.808)。我们没有发现临床特征之间的治疗相互作用,但我们发现了几种生物标志物与罗氟司特之间的相互作用。基于生物标志物的总和评分模型包括 TNF-R1α、ST2、WAP 四硫键核心域蛋白 HE4(WAP-4C)和总胆固醇,评分范围在 0 到 4 之间。在评分 4 分的患者(TNF-R1α、ST2、WAP-4C 升高且总胆固醇低)中,使用罗氟司特治疗是有益的(HR 0.61,95%CI 0.40-0.92,p=0.019)。在评分 0 分的患者中,使用罗氟司特治疗是有害的(HR 5.52,95%CI 1.68-18.13,p=0.005;治疗评分交互作用 p<0.001)。内部验证估计了相似的危险比估计值(0 分:HR 5.56,95%CI 5.27-7-5.87;1 分:HR 1.31,95%CI 1.25-1.33;2 分:HR 0.75,95%CI 0.74-0.76;3 分:HR 1.13,95%CI 1.11-1.15;4 分:HR 0.61,95%CI 0.61-0.62)与原始数据相比。
生物标志物优于临床特征,可用于研究急性心力衰竭的治疗异质性。