Tran Tara T T, Pease Anthony, Wood Anna J, Zajac Jeffrey D, Mårtensson Johan, Bellomo Rinaldo, Ekinci Elif I I
Department of Endocrinology, Austin Health, Melbourne, VIC, Australia.
Department of Medicine, Austin Health, University of Melbourne, Melbourne, VIC, Australia.
Front Endocrinol (Lausanne). 2017 Jun 13;8:106. doi: 10.3389/fendo.2017.00106. eCollection 2017.
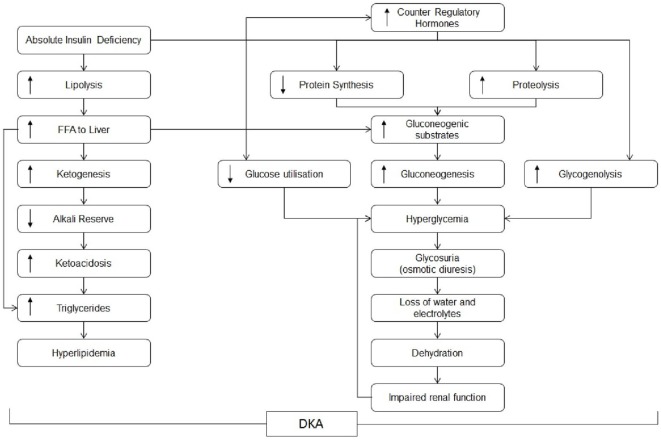
Diabetic ketoacidosis (DKA) is an endocrine emergency with associated risk of morbidity and mortality. Despite this, DKA management lacks strong evidence due to the absence of large randomised controlled trials (RCTs).
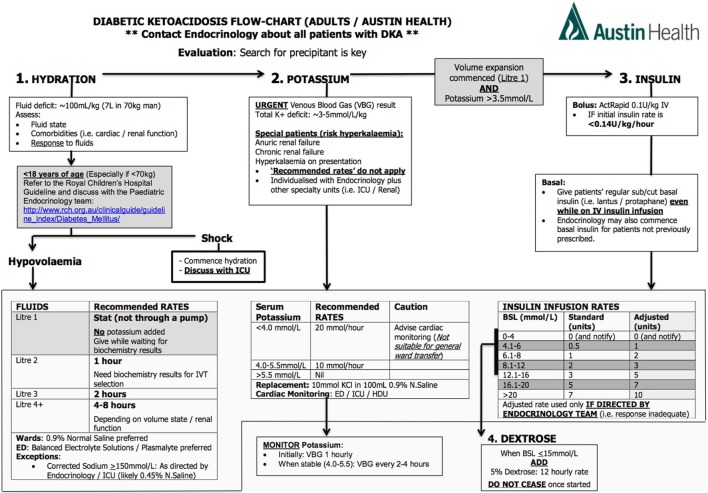
To review existing studies investigating inpatient DKA management in adults, focusing on intravenous (IV) fluids; insulin administration; potassium, bicarbonate, and phosphate replacement; and DKA management protocols and impact of DKA resolution rates on outcomes.
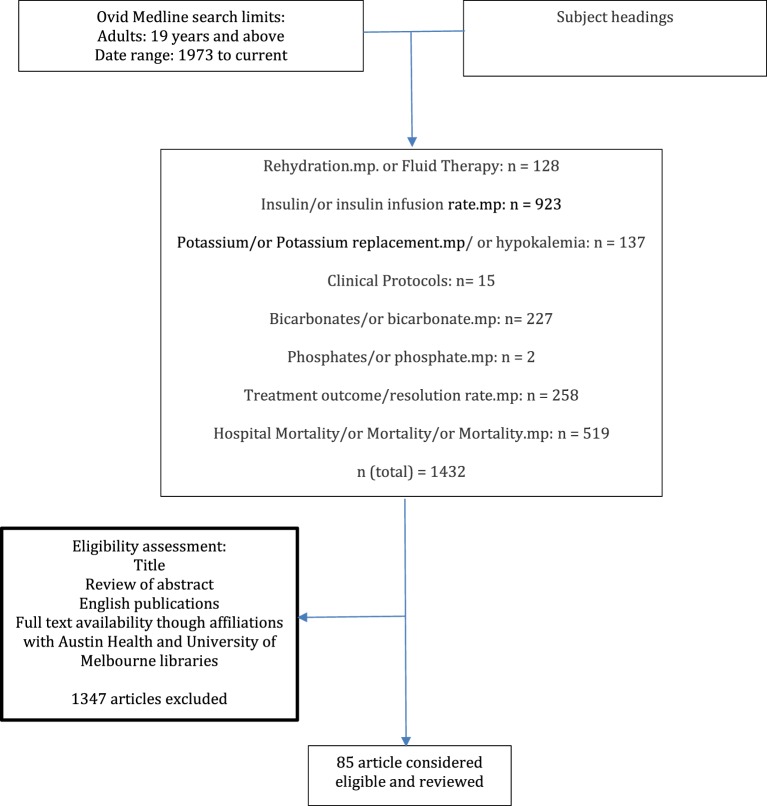
Ovid Medline searches were conducted with limits "all adult" and published between "1973 to current" applied. National consensus statements were also reviewed. Eligibility was determined by two reviewers' assessment of title, abstract, and availability.
A total of 85 eligible articles published between 1973 and 2016 were reviewed. The salient findings were (i) Crystalloids are favoured over colloids though evidence is lacking. The preferred crystalloid and hydration rates remain contentious. (ii) IV infusion of regular human insulin is preferred over the subcutaneous route or rapid acting insulin analogues. Administering an initial IV insulin bolus before low-dose insulin infusions obviates the need for supplemental insulin. Consensus-statements recommend fixed weight-based over "sliding scale" insulin infusions although evidence is weak. (iii) Potassium replacement is imperative although no trials compare replacement rates. (iv) Bicarbonate replacement offers no benefit in DKA with pH > 6.9. In severe metabolic acidosis with pH < 6.9, there is lack of both data and consensus regarding bicarbonate administration. (v) There is no evidence that phosphate replacement offers outcome benefits. Guidelines consider replacement appropriate in patients with cardiac dysfunction, anaemia, respiratory depression, or phosphate levels <0.32 mmol/L. (vi) Upon resolution of DKA, subcutaneous insulin is recommended with IV insulin infusions ceased with an overlap of 1-2 h. (vii) DKA resolution rates are often used as end points in studies, despite a lack of evidence that rapid resolution improves outcome. (viii) Implementation of DKA protocols lacks strong evidence for adherence but may lead to improved clinical outcomes.
There are major deficiencies in evidence for optimal management of DKA. Current practice is guided by weak evidence and consensus opinion. All aspects of DKA management require RCTs to affirm or redirect management and formulate consensus evidence-based practice to improve patient outcomes.
糖尿病酮症酸中毒(DKA)是一种内分泌急症,伴有发病和死亡风险。尽管如此,由于缺乏大型随机对照试验(RCT),DKA的管理缺乏有力证据。
回顾现有关于成人住院患者DKA管理的研究,重点关注静脉输液;胰岛素给药;钾、碳酸氢盐和磷酸盐补充;以及DKA管理方案和DKA缓解率对预后的影响。
在Ovid Medline数据库中进行检索,限定为“所有成人”,并应用“1973年至当前”发表的文献。还查阅了国家共识声明。由两位审稿人根据标题、摘要和可获取性来确定入选资格。
共回顾了1973年至2016年间发表的85篇符合条件的文章。主要发现如下:(i)尽管缺乏证据,但晶体液比胶体液更受青睐。首选的晶体液和补液速度仍存在争议。(ii)静脉输注正规人胰岛素优于皮下给药途径或速效胰岛素类似物。在低剂量胰岛素输注前给予初始静脉胰岛素推注可避免补充胰岛素的需要。共识声明推荐基于固定体重的胰岛素输注而非“滑动比例”胰岛素输注,尽管证据不足。(iii)钾补充必不可少,尽管没有试验比较补充率。(iv)对于pH>6.9的DKA患者,补充碳酸氢盐无益处。对于pH<6.9的严重代谢性酸中毒患者,关于碳酸氢盐给药既缺乏数据也未达成共识。(v)没有证据表明补充磷酸盐对预后有益。指南认为对于有心脏功能障碍、贫血、呼吸抑制或磷酸盐水平<0.32 mmol/L的患者补充是合适的。(vi)DKA缓解后,建议皮下注射胰岛素,静脉胰岛素输注停止,两者重叠1 - 2小时。(vii)尽管缺乏证据表明快速缓解能改善预后,但DKA缓解率在研究中常被用作终点。(viii)DKA方案的实施缺乏关于依从性的有力证据,但可能导致临床预后改善。
DKA最佳管理的证据存在重大缺陷。当前的实践以薄弱的证据和共识意见为指导。DKA管理的各个方面都需要RCT来确认或调整管理方式,并制定基于共识证据的实践方法以改善患者预后。