Schulman Ariel A, Howard Lauren E, Tay Kae Jack, Tsivian Efrat, Sze Christina, Amling Christopher L, Aronson William J, Cooperberg Matthew R, Kane Christopher J, Terris Martha K, Freedland Stephen J, Polascik Thomas J
Division of Urology, Duke University Medical Center, Durham, North Carolina.
Surgery Section, Durham Veterans Affairs Medical Center, Durham, North Carolina.
Cancer. 2017 Nov 1;123(21):4122-4129. doi: 10.1002/cncr.30844. Epub 2017 Jun 29.
A 5-tier prognostic grade group (GG) system was enacted to simplify the risk stratification of patients with prostate cancer in which Gleason scores of ≤6, 3 + 4, 4 + 3, 8, and 9 or 10 are considered GG 1 through 5, respectively. The authors investigated the utility of biopsy GG for predicting long-term oncologic outcomes after radical prostatectomy in an equal-access health system.
Men who underwent prostatectomy at 1 of 6 Veterans Affairs hospitals in the Shared Equal Access Regional Cancer Hospital database between 2005 and 2015 were reviewed. The prognostic ability of biopsy GG was examined using Cox models. Interactions between GG and race also were tested.
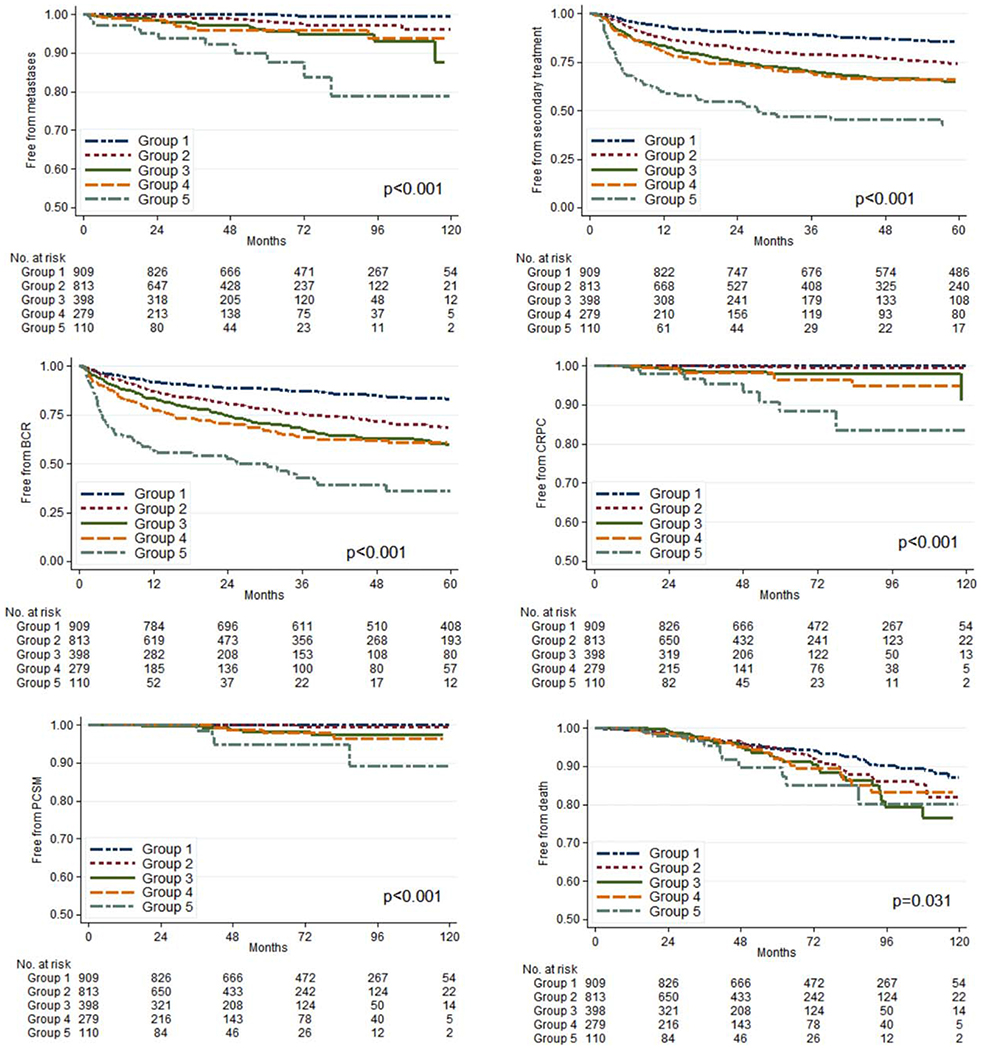
In total, 2509 men were identified who had data available on biopsy Gleason scores, covariates, and follow-up. The cohort included men with GG 1 (909 patients; 36.2%), GG 2 (813 patients; 32.4%), GG 3 (398 patients; 15.9%), GG 4 (279 patients; 11.1%), and GG 5 (110 patients; 4.4%) prostate cancer. The cohort included 1002 African American men (41%). The median follow-up was 60 months (interquartile range, 33-90 months). Higher GG was associated with higher clinical stage, older age, more recent surgery, and surgical center (P < .001) as well as increased biochemical recurrence, secondary therapy, castration-resistant prostate cancer, metastases, and prostate cancer-specific mortality (all P < .001). There were no significant interactions with race in predicting measured outcomes.
The 5-tier GG system predicted multiple long-term endpoints after radical prostatectomy in an equal-access health system. The predictive value was consistent across races. Cancer 2017;123:4122-4129. © 2017 American Cancer Society.
制定了一个5级预后分级组(GG)系统,以简化前列腺癌患者的风险分层,其中 Gleason 评分≤6、3 + 4、4 + 3、8以及9或10分别被视为GG 1至5级。作者在一个平等医疗的卫生系统中,研究了活检GG分级对预测根治性前列腺切除术后长期肿瘤学结局的效用。
回顾了2005年至2015年期间在共享平等医疗区域癌症医院数据库中6家退伍军人事务医院之一接受前列腺切除术的男性患者。使用Cox模型检验活检GG分级的预后能力。还测试了GG分级与种族之间的相互作用。
总共确定了2509名男性患者,他们有关于活检Gleason评分、协变量和随访的数据。该队列包括GG 1级(909例患者;36.2%)、GG 2级(813例患者;32.4%)、GG 3级(398例患者;15.9%)、GG 4级(279例患者;11.1%)和GG 5级(110例患者;4.4%)的前列腺癌患者。该队列包括1002名非裔美国男性(41%)。中位随访时间为60个月(四分位间距,33 - 90个月)。较高的GG分级与更高的临床分期、年龄较大、手术时间更近以及手术中心相关(P <.001),同时生化复发、二次治疗、去势抵抗性前列腺癌、转移和前列腺癌特异性死亡率增加(所有P <.001)。在预测测量结局方面,与种族没有显著的相互作用。
在一个平等医疗的卫生系统中,5级GG系统预测了根治性前列腺切除术后的多个长期终点。预测价值在不同种族中是一致的。《癌症》2017年;123:4122 - 4129。© 2017美国癌症协会。