West German Study Group, Ludwig-Weber-Str. 15, 41061, Moenchengladbach, Germany.
Ev. Hospital Bethesda, Breast Center Niederrhein, Ludwig-Weber-Str. 15, 41061, Moenchengladbach, Germany.
Breast Cancer Res Treat. 2017 Oct;165(3):573-583. doi: 10.1007/s10549-017-4358-6. Epub 2017 Jun 29.
The prospective phase 3 PlanB trial used the Oncotype DX Recurrence Score (RS) to define a genomically low-risk subset of clinically high-risk pN0-1 early breast cancer (EBC) patients for treatment with adjuvant endocrine therapy (ET) alone. Here, we report five-year data evaluating the prognostic value of RS, Ki-67, and other traditional clinicopathological parameters.
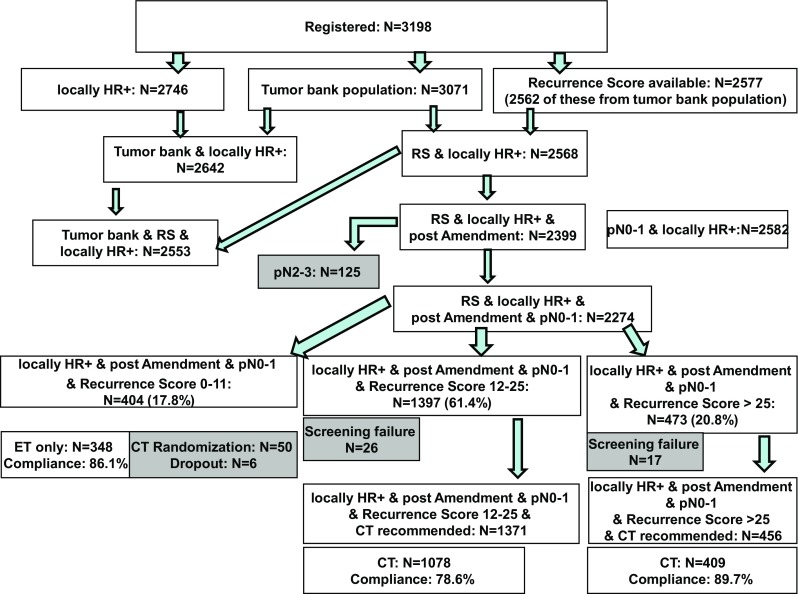
A central tumour bank was prospectively established within PlanB. Following an early amendment, hormone receptor (HR)+ , pN0-1 RS ≤ 11 patients were recommended to omit chemotherapy. Patients with RS ≥ 12, pN2-3, or HR-negative/HER2-negative disease were randomised to anthracycline-containing or anthracycline-free chemotherapy. Primary endpoint: disease-free survival (DFS). PlanB Clinicaltrials.gov identifier: NCT01049425.
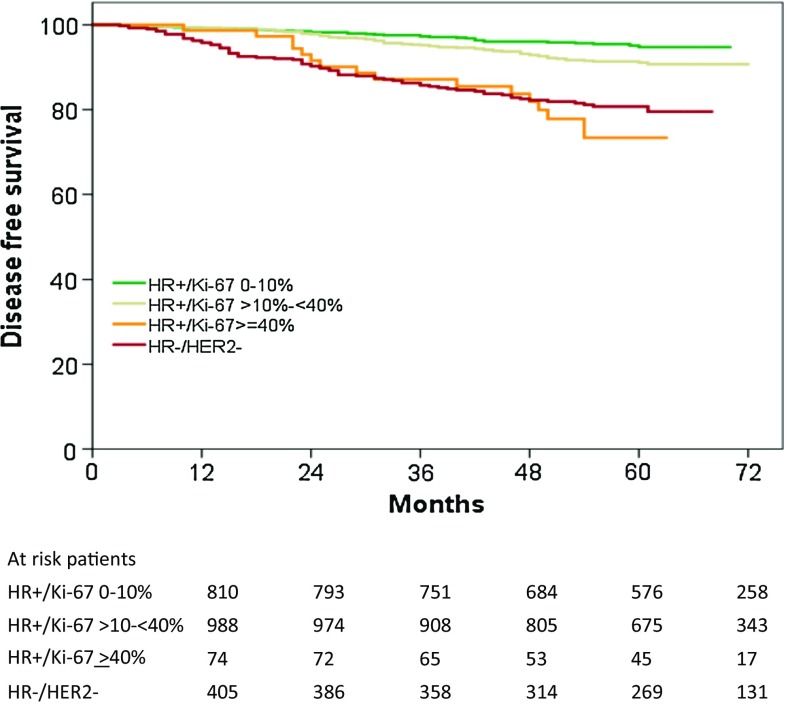
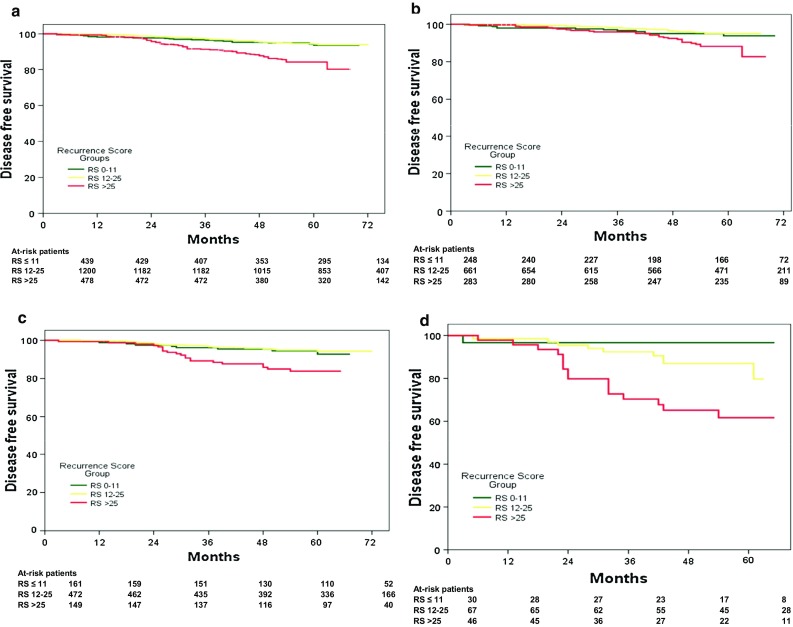
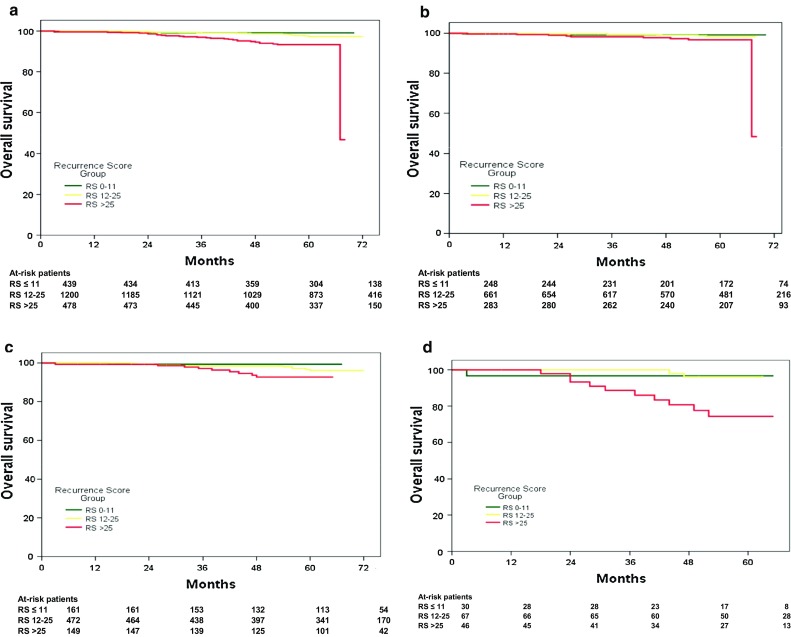
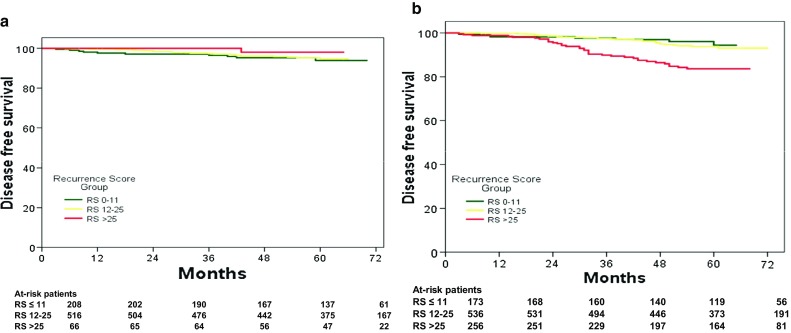
From 2009 to 2011, PlanB enrolled 3198 patients (central tumour bank, n = 3073) with the median age of 56 years, 41.1% pN+, and 32.5% grade 3 EBC. Chemotherapy was omitted in 348/404 (86.1%) eligible RS ≤ 11 patients. After 55 months of median follow-up, five-year DFS in ET-treated RS ≤ 11 patients was 94% (in both pN0 and pN1) versus 94% (RS 12-25) and 84% (RS > 25) in chemotherapy-treated patients (p < 0.001); five-year overall survival (OS) was 99 versus 97% and 93%, respectively (p < 0.001). Nodal status, central/local grade, tumour size, continuous Ki-67, progesterone receptor (PR), IHC4, and RS were univariate prognostic factors for DFS. In a multivariate analysis including all univariate prognostic markers, only pN2-3, central and local grade 3, tumour size >2 cm, and RS, but not IHC4 or Ki-67 were independent adverse factors. If RS was excluded, IHC4 or both Ki-67 and PR entered the model. The impact of RS was particularly pronounced in patients with intermediate Ki-67 (>10%, <40%) tumours.
The excellent five-year outcomes in clinically high-risk, genomically low-risk (RS ≤ 11) pN0-1 patients without adjuvant chemotherapy support using RS with standardised pathology for treatment decisions in HR+ HER2-negative EBC. Ki-67 has the potential to support patient selection for genomic testing.
前瞻性 3 期 PlanB 试验使用 Oncotype DX 复发评分(RS)来定义临床高危 pN0-1 早期乳腺癌(EBC)患者的基因组低度危险亚组,以便单独接受辅助内分泌治疗(ET)。在此,我们报告了评估 RS、Ki-67 和其他传统临床病理参数的预后价值的 5 年数据。
在 PlanB 中,前瞻性地建立了一个中央肿瘤库。在早期修正案之后,建议激素受体(HR)+、pN0-1 RS≤11 的患者省略化疗。RS≥12、pN2-3 或 HR 阴性/HER2 阴性疾病的患者被随机分配到含蒽环类药物或无蒽环类药物的化疗中。主要终点:无病生存(DFS)。PlanB Clinicaltrials.gov 标识符:NCT01049425。
2009 年至 2011 年,PlanB 招募了 3198 名患者(中央肿瘤库,n=3073),中位年龄为 56 岁,41.1%pN+,32.5%为 3 级 EBC。404 名符合条件的 RS≤11 患者中,有 348 名(86.1%)省略了化疗。在中位随访 55 个月后,ET 治疗 RS≤11 患者的 5 年 DFS 为 94%(在 pN0 和 pN1 中),而化疗治疗患者的 5 年 DFS 为 94%(RS 12-25)和 84%(RS>25)(p<0.001);5 年总生存(OS)分别为 99%和 97%和 93%(p<0.001)。淋巴结状态、中央/局部分级、肿瘤大小、连续 Ki-67、孕激素受体(PR)、IHC4 和 RS 是 DFS 的单因素预后因素。在包括所有单因素预后标志物的多变量分析中,只有 pN2-3、中央和局部 3 级、肿瘤大小>2cm 和 RS,但不是 IHC4 或 Ki-67 是独立的不良因素。如果排除 RS,IHC4 或 Ki-67 和 PR 都会进入模型。RS 的影响在具有中等 Ki-67(>10%,<40%)肿瘤的临床高危、基因组低度危险(RS≤11)pN0-1 患者中尤为显著。
在没有辅助化疗的情况下,临床高危、基因组低度危险(RS≤11)pN0-1 患者的 5 年良好结果支持使用标准化病理学进行 RS 治疗决策。Ki-67 具有支持基因组检测患者选择的潜力。