Ingelbeen Brecht, Bah Elhadj Ibrahima, Decroo Tom, Balde Idrissa, Nordenstedt Helena, van Griensven Johan, De Weggheleire Anja
Médecins Sans Frontières, Operational Centre Brussels, Conakry, Guinea.
Centre Hospitalier Universitaire de Donka, Conakry, Guinea.
PLoS One. 2017 Jun 30;12(6):e0180070. doi: 10.1371/journal.pone.0180070. eCollection 2017.
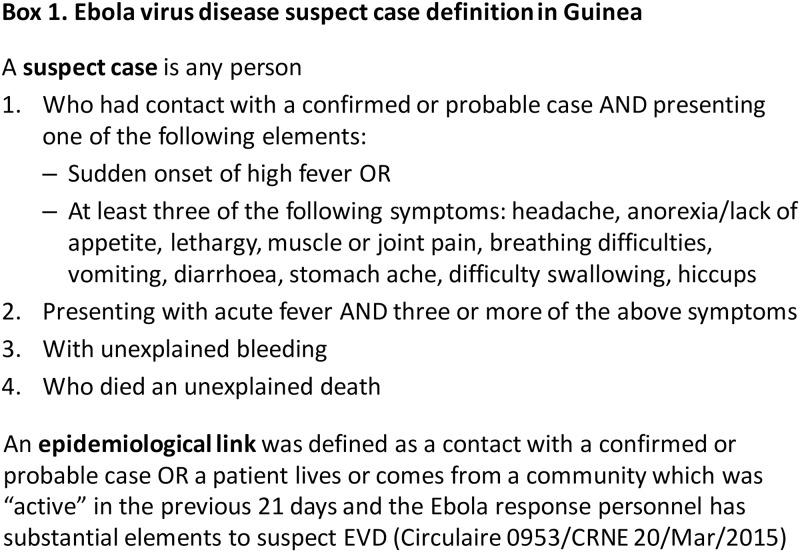
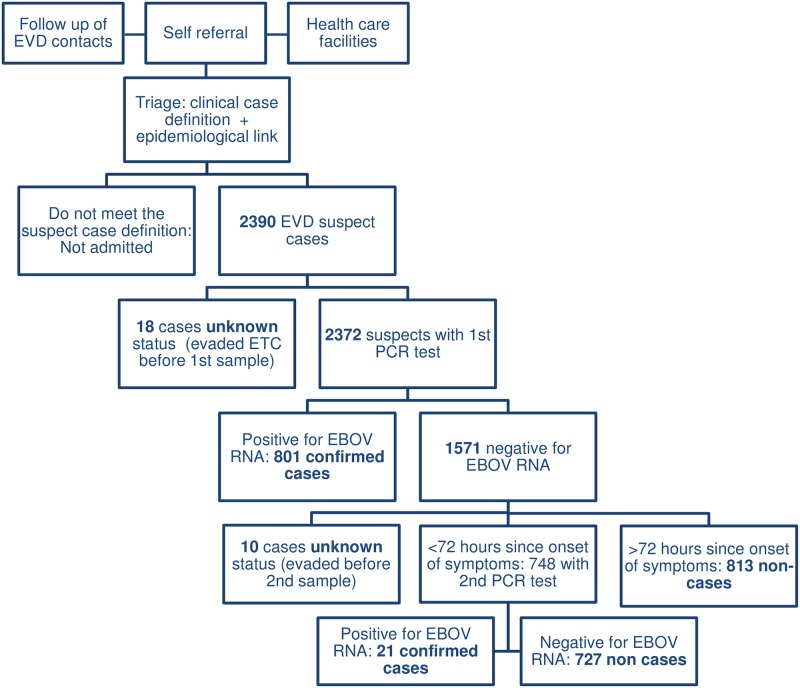
Non-cases are suspect Ebola Virus Disease (EVD) cases testing negative by EVD RT-PCR after admission to an Ebola Treatment Centre (ETC). Admitting non-cases to an ETC prompts concerns on case- and workload in the ETC, risk for nosocomial EVD infection, and delays in diagnosis and disease-specific treatment. We retrospectively analysed characteristics, outcomes and determinants of death of EVD cases and non-cases admitted to the Conakry ETC in Guinea between 03/2014 and 09/2015. Of the 2362 admitted suspects who underwent full confirmatory PCR testing, 1540 (65.2%) were non-cases; among them 727 needed repeated confirmatory PCR testing resulting in 2.5 days (average) in the ETC isolation ward. Twenty-one patients tested positive on the repeat test, most in a period of flawed sampling for the initial test and none after introduction of PCR confirmation with geneXpert. No readmissions following nosocomial EVD infection were recorded. No combination of symptoms yielded acceptable sensitivity and specificity to allow differentiating confirmed from non-cases. Symptoms as ocular bleeding/redness have high specificity, but limited usefulness as not common. Admission delay and age distribution were not different for both groups. In total, 98 (20.6%) of 475 deaths in the ETC were non-cases. Most died within 24 hours after admission. Living in Conakry (aOR 1.78 (1.08-2.96)) was the strongest risk factor for death. Weeks with higher admission load had lower case fatality among non-cases, probably because more acute (and treatable) illnesses of contacts of known cases were admitted. These findings show high numbers of potentially critically ill non-cases need to be considered when setting up triage and referral of EVD suspect cases. Symptoms and risk factors alone do not allow differentiating the non-cases. Integration of highly-sensitive EVD diagnostic methods with short turnaround time in the triage of peripheral hospitals and dropping the systematic 2nd PCR for symptomatic early presenters could limit delays in access to adapted care of cases and seriously ill non-cases. Whether feasible without compromising outbreak control, and under which conditions, should be further assessed.
非病例是指在被收治到埃博拉治疗中心(ETC)后,经埃博拉病毒病(EVD)逆转录聚合酶链反应(RT-PCR)检测呈阴性的疑似埃博拉病毒病病例。将非病例收治到ETC引发了对ETC病例数量和工作量、医院内埃博拉病毒病感染风险以及诊断和针对性治疗延迟等问题的担忧。我们回顾性分析了2014年3月至2015年9月期间收治到几内亚科纳克里ETC的埃博拉病毒病病例和非病例的特征、结局及死亡决定因素。在2362名接受全面确诊PCR检测的收治疑似病例中,1540例(65.2%)为非病例;其中727例需要重复进行确诊PCR检测,在ETC隔离病房平均停留2.5天。21例患者在重复检测时呈阳性,大多数出现在初次检测采样有缺陷的时期,在引入GeneXpert PCR确诊后无一例阳性。未记录到医院内埃博拉病毒病感染后的再次入院情况。没有任何症状组合能产生可接受的敏感性和特异性以区分确诊病例和非病例。眼部出血/发红等症状具有较高的特异性,但因不常见而实用性有限。两组的入院延迟和年龄分布无差异。在ETC的475例死亡病例中,共有98例(20.6%)为非病例。大多数在入院后24小时内死亡。居住在科纳克里(调整后比值比1.78(1.08 - 2.96))是最强的死亡风险因素。入院负荷较高的几周内,非病例的病死率较低,可能是因为收治了更多已知病例接触者中更急性(且可治疗)的疾病患者。这些研究结果表明,在制定埃博拉病毒病疑似病例的分诊和转诊方案时,需要考虑大量可能病情危急的非病例。仅靠症状和风险因素无法区分非病例。在外围医院分诊中整合周转时间短的高灵敏度埃博拉病毒病诊断方法,并取消对有症状早期就诊者进行系统性二次PCR检测,可能会减少病例和重症非病例获得适当治疗的延迟。在不影响疫情控制的情况下是否可行以及在何种条件下可行,应进一步评估。