Mutagonda Ritah F, Kamuhabwa Appolinary A R, Minzi Omary M S, Massawe Siriel N, Asghar Muhammad, Homann Manijeh V, Färnert Anna, Aklillu Eleni
Department of Clinical Pharmacy and Pharmacology, School of Pharmacy, Muhimbili University of Health and Allied Sciences, P.O. Box 65013, Dar es Salaam, Tanzania.
Department of Obstetrics and Gynaecology, School of Medicine, Muhimbili University of Allied Sciences, P.O Box 65013, Dar es Salaam, Tanzania.
Malar J. 2017 Jul 3;16(1):267. doi: 10.1186/s12936-017-1914-9.
Pregnancy has considerable effects on the pharmacokinetic properties of drugs used to treat uncomplicated Plasmodium falciparum malaria. The role of pharmacogenetic variation on anti-malarial drug disposition and efficacy during pregnancy is not well investigated. The study aimed to examine the effect of pharmacogenetics on lumefantrine (LF) pharmacokinetics and treatment outcome in pregnant women.
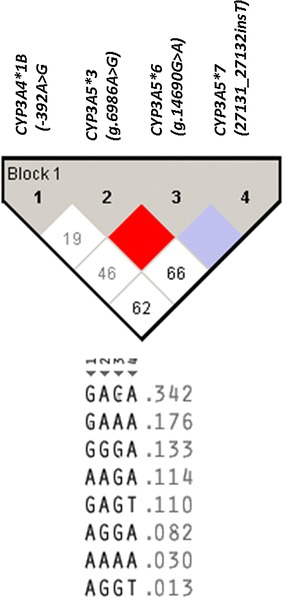
Pregnant women with uncomplicated falciparum malaria were enrolled and treated with artemether-lumefantrine (ALu) at Mkuranga and Kisarawe district hospitals in Coast Region of Tanzania. Day-7 LF plasma concentration and genotyping forCYP2B6 (c.516G>T, c.983T>C), CYP3A4*1B, CYP3A5 (*3, *6, *7) and ABCB1 c.4036A4G were determined. Blood smear for parasite quantification by microscopy, and dried blood spot for parasite screening and genotyping using qPCR and nested PCR were collected at enrolment up to day 28 to differentiate between reinfection from recrudescence. Treatment response was recorded following the WHO protocol.
In total, 92 pregnant women in their second and third trimester were included in the study and 424 samples were screened for presence of P. falciparum. Parasites were detected during the follow up period in 11 (12%) women between day 7 and 28 after treatment and PCR genotyping confirmed recrudescent infection in 7 (63.3%) women. The remaining four (36.4%) pregnant women had reinfection: one on day 14 and three on day 28. The overall PCR-corrected treatment failure rate was 9.0% (95% CI 4.4-17.4). Day 7 LF concentration was not significantly influenced by CYP2B6, CYP3A41B and ABCB1 c.4036A>G genotypes. Significant associations between CYP3A5 genotype and day 7 plasma LF concentrations was found, being higher in carriers of CYP3A5 defective variant alleles than CYP3A51/1 genotype. No significant influence of CYP2B6, CYP3A5 and ABCB1 c.4036A>Genotypes on malaria treatment outcome were observed. However, CYP3A41B did affect malaria treatment outcome in pregnant women followed up for 28 days (P = 0.018).
Genetic variations in CYP3A4 and CYP3A5may influence LF pharmacokinetics and treatment outcome in pregnant women.
妊娠对用于治疗非复杂性恶性疟原虫疟疾的药物的药代动力学特性有相当大的影响。药物遗传学变异在妊娠期间抗疟药物处置和疗效中的作用尚未得到充分研究。本研究旨在探讨药物遗传学对孕妇中卤泛群(LF)药代动力学和治疗结果的影响。
在坦桑尼亚沿海地区的姆库兰加和基萨拉韦区医院,招募患有非复杂性恶性疟的孕妇并用蒿甲醚-卤泛群(ALu)进行治疗。测定第7天的LF血浆浓度以及CYP2B6(c.516G>T,c.983T>C)、CYP3A4*1B、CYP3A5(*3、*6、*7)和ABCB1 c.4036A4G的基因分型。在入组时直至第28天采集血涂片通过显微镜进行寄生虫定量,并采集干血斑用于使用qPCR和巢式PCR进行寄生虫筛查和基因分型,以区分再感染和复发。按照世界卫生组织的方案记录治疗反应。
总共92名孕中期和孕晚期孕妇纳入本研究,共筛查424份样本以检测恶性疟原虫的存在。在治疗后第7天至28天期间,11名(12%)妇女在随访期间检测到寄生虫,PCR基因分型证实7名(63.3%)妇女为复发感染。其余4名(36.4%)孕妇为再感染:1名在第14天,3名在第28天。经PCR校正后的总体治疗失败率为9.0%(95%CI 4.4-17.4)。第7天的LF浓度不受CYP2B6、CYP3A41B和ABCB1 c.4036A>G基因型的显著影响。发现CYP3A5基因型与第7天血浆LF浓度之间存在显著关联,CYP3A5缺陷变异等位基因携带者的浓度高于CYP3A51/1基因型。未观察到CYP2B6、CYP3A5和ABCB1 c.4036A>G基因型对疟疾治疗结果有显著影响。然而,CYP3A41B确实影响了随访28天的孕妇的疟疾治疗结果(P = 0.018)。
CYP3A4和CYP3A5的基因变异可能影响孕妇中LF的药代动力学和治疗结果。