Carrillo Elena, Lomas Amparo, Pinés Pedro J, Lamas Cristina
Endocrinologists in Complejo Hospitalario Universitario de Albacete, Castilla La ManchaSpain.
Endocrinol Diabetes Metab Case Rep. 2017 Jun 23;2017. doi: 10.1530/EDM-17-0052. eCollection 2017.
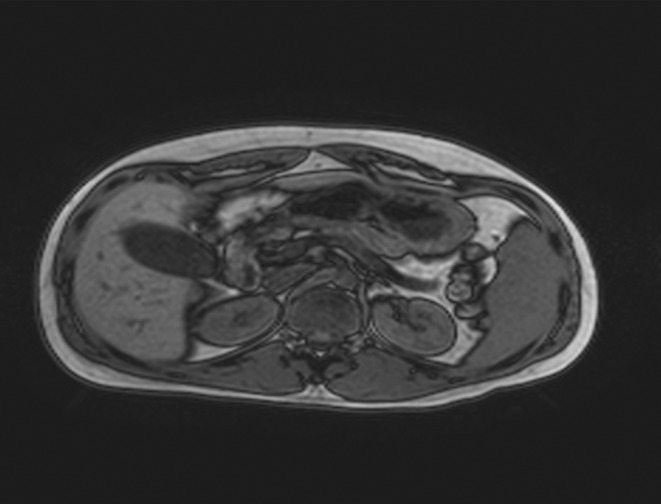
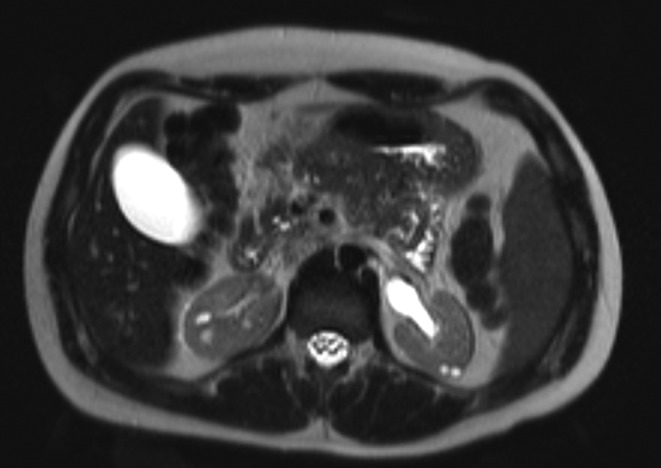
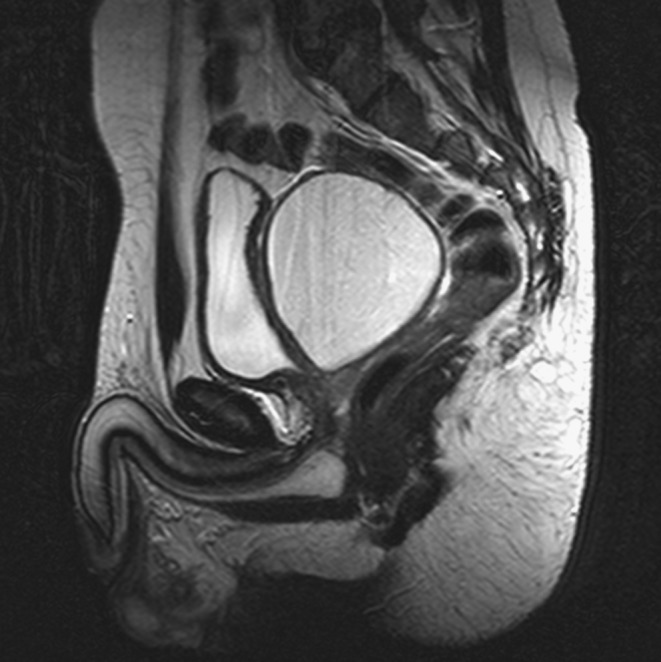
Mutations in hepatocyte nuclear factor 1β gene () are responsible for a multisystemic syndrome where monogenic diabetes (classically known as MODY 5) and renal anomalies, mostly cysts, are the most characteristic findings. Urogenital malformations, altered liver function tests, hypomagnesemia or hyperuricemia and gout are also part of the syndrome. Diabetes in these patients usually requires early insulinization. We present the case of a young non-obese male patient with a personal history of renal multicystic dysplasia and a debut of diabetes during adolescence with simple hyperglycemia, negative pancreatic autoimmunity and detectable C-peptide levels. He also presented epididymal and seminal vesicle cysts, hypertransaminasemia, hyperuricemia and low magnesium levels. In the light of these facts we considered the possibility of a mutation. The sequencing study of this gene confirmed a heterozygous mutation leading to a truncated and less functional protein. Genetic studies of his relatives were negative; consequently, it was classified as a mutation. In particular, our patient maintained good control of his diabetes on oral antidiabetic agents for a long period of time. He eventually needed insulinization although oral therapy was continued alongside, allowing reduction of prandial insulin requirements. The real prevalence of mutations in is probably underestimated owing to a wide phenotypical variability. As endocrinologists, we should consider this possibility in young non-obese diabetic patients with a history of chronic non-diabetic nephropathy, especially in the presence of some of the other characteristic manifestations.
mutations are a rare cause of monogenic diabetes, often being a part of a multisystemic syndrome.The combination of young-onset diabetes and genitourinary anomalies with slowly progressive nephropathy of non-diabetic origin in non-obese subjects should rise the suspicion of such occurrence. A family history may not be present.Once diagnosis is made, treatment of diabetes with oral agents is worth trying, since the response can be sustained for a longer period than the one usually described. Oral treatment can help postpone insulinization and, once this is necessary, can help reduce the required doses.
肝细胞核因子1β基因()突变可导致一种多系统综合征,其中单基因糖尿病(经典的称为MODY 5)和肾脏异常(主要是囊肿)是最典型的表现。泌尿生殖系统畸形、肝功能检查异常、低镁血症或高尿酸血症及痛风也是该综合征的一部分。这些患者的糖尿病通常需要早期胰岛素治疗。我们报告一例年轻非肥胖男性患者,有肾多囊性发育不良个人史,青春期首次出现糖尿病,表现为单纯高血糖、胰腺自身抗体阴性且C肽水平可检测。他还出现附睾和精囊囊肿、转氨酶升高、高尿酸血症及低镁水平。鉴于这些情况,我们考虑了突变的可能性。该基因的测序研究证实存在杂合突变,导致蛋白质截短且功能降低。对其亲属的基因研究为阴性;因此,该突变被归类为突变。特别是,我们的患者长期口服降糖药能很好地控制糖尿病。尽管同时继续口服治疗,但他最终仍需要胰岛素治疗,这使得餐时胰岛素需求量减少。由于表型变异性广泛,突变的实际患病率可能被低估。作为内分泌科医生,我们应在有慢性非糖尿病肾病病史的年轻非肥胖糖尿病患者中考虑这种可能性,尤其是存在一些其他典型表现时。
突变是单基因糖尿病的罕见病因,常是多系统综合征的一部分。非肥胖个体中,青少年起病的糖尿病、泌尿生殖系统异常与非糖尿病性缓慢进展性肾病的组合应引起对此类情况的怀疑。可能无家族史。一旦确诊,值得尝试用口服药物治疗糖尿病,因为其反应可持续较长时间,比通常描述的时间更长。口服治疗有助于推迟胰岛素治疗,一旦需要胰岛素治疗,可帮助减少所需剂量。