Fuchs Charles S, Muro Kei, Tomasek Jiri, Van Cutsem Eric, Cho Jae Yong, Oh Sang-Cheul, Safran Howard, Bodoky György, Chau Ian, Shimada Yasuhiro, Al-Batran Salah-Eddin, Passalacqua Rodolfo, Ohtsu Atsushi, Emig Michael, Ferry David, Chandrawansa Kumari, Hsu Yanzhi, Sashegyi Andreas, Liepa Astra M, Wilke Hansjochen
Dana-Farber Cancer Institute, Boston, MA, USA.
Department of Clinical Oncology, Aichi Cancer Center Hospital, Nagoya, Japan.
J Gastric Cancer. 2017 Jun;17(2):132-144. doi: 10.5230/jgc.2017.17.e16. Epub 2017 Jun 16.
To identify baseline prognostic factors for survival in patients with disease progression, during or after chemotherapy for the treatment of advanced gastric or gastroesophageal junction (GEJ) cancer.
We pooled data from patients randomized between 2009 and 2012 in 2 phase III, global double-blind studies of ramucirumab for the treatment of advanced gastric or GEJ adenocarcinoma following disease progression on first-line platinum- and/or fluoropyrimidine-containing therapy (REGARD and RAINBOW). Forty-one key baseline clinical and laboratory factors common in both studies were examined. Model building started with covariate screening using univariate Cox models (significance level=0.05). A stepwise multivariable Cox model identified the final prognostic factors (entry+exit significance level=0.01). Cox models were stratified by treatment and geographic region. The process was repeated to identify baseline prognostic quality of life (QoL) parameters.
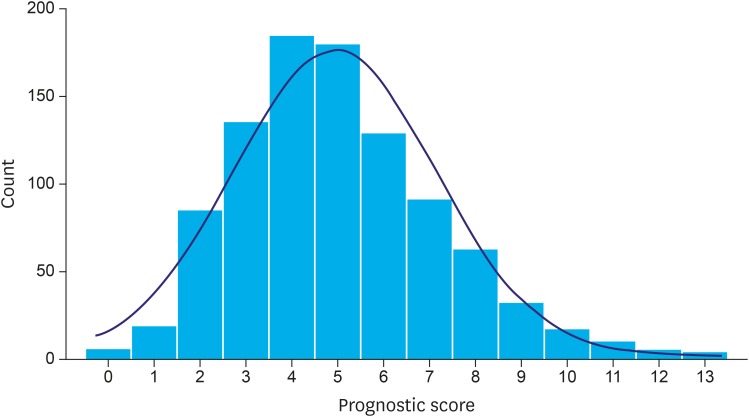
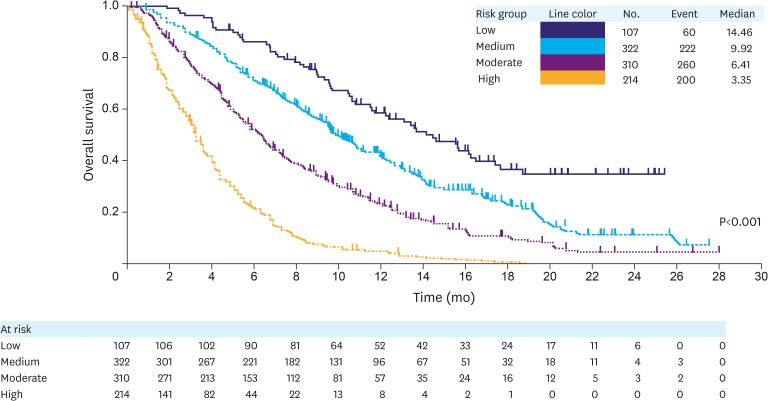
Of 1,020 randomized patients, 953 (93%) patients without any missing covariates were included in the analysis. We identified 12 independent prognostic factors of poor survival: 1) peritoneal metastases; 2) Eastern Cooperative Oncology Group (ECOG) performance score 1; 3) the presence of a primary tumor; 4) time to progression since prior therapy <6 months; 5) poor/unknown tumor differentiation; abnormally low blood levels of 6) albumin, 7) sodium, and/or 8) lymphocytes; and abnormally high blood levels of 9) neutrophils, 10) aspartate aminotransferase (AST), 11) alkaline phosphatase (ALP), and/or 12) lactate dehydrogenase (LDH). Factors were used to devise a 4-tier prognostic index (median overall survival [OS] by risk [months]: high=3.4, moderate=6.4, medium=9.9, and low=14.5; Harrell's C-index=0.66; 95% confidence interval [CI], 0.64-0.68). Addition of QoL to the model identified patient-reported appetite loss as an independent prognostic factor.
The identified prognostic factors and the reported prognostic index may help clinical decision-making, patient stratification, and planning of future clinical studies.
确定晚期胃癌或胃食管交界(GEJ)癌患者在化疗期间或化疗后疾病进展时生存的基线预后因素。
我们汇总了2009年至2012年期间在两项全球双盲III期研究中随机分组的患者数据,这两项研究均为雷莫西尤单抗用于治疗一线含铂和/或氟嘧啶治疗后疾病进展的晚期胃或GEJ腺癌(REGARD和RAINBOW)。对两项研究中常见的41个关键基线临床和实验室因素进行了检查。模型构建首先使用单变量Cox模型进行协变量筛选(显著性水平=0.05)。逐步多变量Cox模型确定了最终的预后因素(纳入+排除显著性水平=0.01)。Cox模型按治疗和地理区域进行分层。重复该过程以确定基线预后生活质量(QoL)参数。
在1020例随机分组的患者中,953例(93%)无任何协变量缺失的患者纳入分析。我们确定了12个生存不良的独立预后因素:1)腹膜转移;2)东部肿瘤协作组(ECOG)体能状态评分1;3)存在原发性肿瘤;4)自 prior therapy 以来的疾病进展时间<6个月;5)肿瘤分化差/未知;血液中6)白蛋白、7)钠和/或8)淋巴细胞水平异常低;以及血液中9)中性粒细胞、10)天冬氨酸转氨酶(AST)、11)碱性磷酸酶(ALP)和/或12)乳酸脱氢酶(LDH)水平异常高。这些因素用于设计一个4级预后指数(按风险分层的中位总生存期[OS] [月]:高=3.4,中=6.4,中低=9.9,低=14.5;Harrell's C指数=0.66;95%置信区间[CI],0.64 - 0.68)。将QoL纳入模型确定患者报告的食欲减退为独立预后因素。
所确定的预后因素和报告的预后指数可能有助于临床决策、患者分层以及未来临床研究的规划。