Amilcare Parisi, Francesco Ricci, Alessandro Gemini, Stefano Trastulli, Roberto Cirocchi, Jacopo Desiderio, Department of Digestive Surgery, St. Mary's Hospital of Terni, University of Perugia, 05100 Terni, Italy.
World J Gastroenterol. 2017 Jun 21;23(23):4293-4302. doi: 10.3748/wjg.v23.i23.4293.
To show outcomes of our series of patients that underwent a total gastrectomy with a robotic approach and highlight the technical details of a proposed solution for the reconstruction phase.
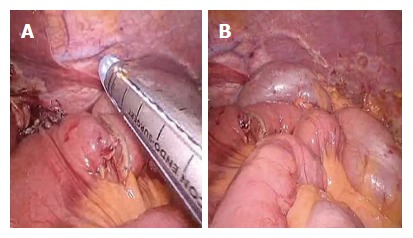
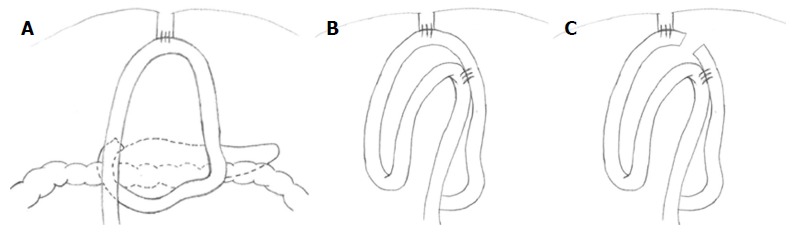
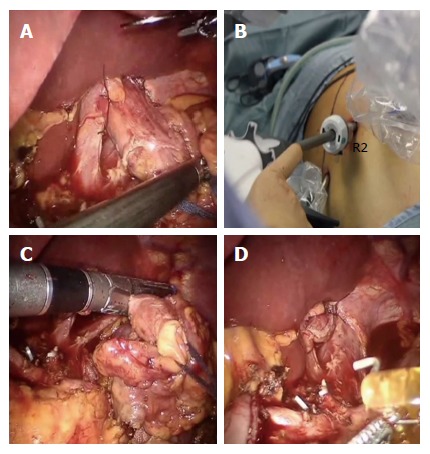
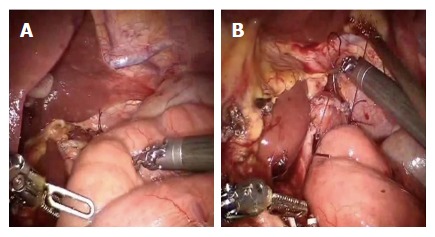
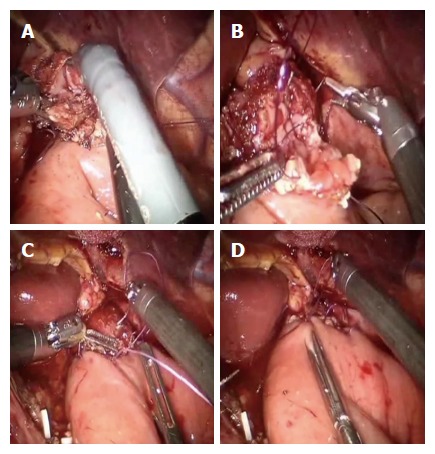
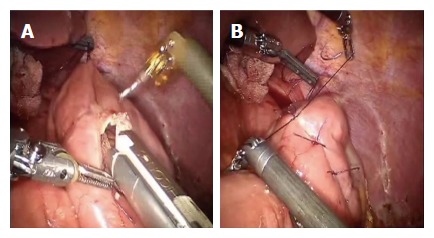
Data of gastrectomies performed from May 2014 to October 2016, were extracted and analyzed. Basic characteristics of patients, surgical and clinical outcomes were reported. The technique for reconstruction (Parisi Technique) consists on a loop of bowel shifted up antecolic to directly perform the esophago-enteric anastomosis followed by a second loop, measured up to 40 cm starting from the esojejunostomy, fixed to the biliary limb to create an enteroenteric anastomosis. The continuity between the two anastomoses is interrupted just firing a linear stapler, so obtaining the Roux-en-Y by avoiding to interrupt the mesentery.
Fifty-five patients were considered in the present analysis. Estimated blood loss was 126.55 ± 73 mL, no conversions to open surgery occurred, R0 resections were obtained in all cases. Hospital stay was 5 (3-17) d, no anastomotic leakage occurred. Overall, a fast functional recovery was shown with a median of 3 (3-6) d in starting a solid diet.
Robotic surgery and the adoption of a tailored reconstruction technique have increased the feasibility and safety of a minimally invasive approach for total gastrectomy. The present series of patients shows its implementation in a western center with satisfying short-term outcomes.
展示我们一系列接受机器人全胃切除术患者的结果,并强调重建阶段提出的解决方案的技术细节。
提取并分析了 2014 年 5 月至 2016 年 10 月期间进行的胃切除术的数据。报告了患者的基本特征、手术和临床结果。重建技术(帕里西技术)包括将肠袢向前结肠移位,直接进行食管-肠吻合术,然后测量距食管空肠吻合术 40cm 处的第二个肠袢,将其固定在胆管支上以形成肠肠吻合术。通过仅启动线性吻合器中断两个吻合口之间的连续性,从而避免中断肠系膜来获得 Roux-en-Y。
本分析共纳入 55 例患者。估计出血量为 126.55±73ml,无中转开腹手术,所有病例均行 R0 切除。住院时间为 5(3-17)d,无吻合口漏。总体而言,中位时间为 3(3-6)d 即可开始摄入固体饮食,患者快速恢复了功能。
机器人手术和采用量身定制的重建技术提高了微创全胃切除术的可行性和安全性。本系列患者展示了其在西方中心的实施情况,具有令人满意的短期结果。