van Helden E J, Menke-van der Houven van Oordt C W, Heymans M W, Ket J C F, van den Oord R, Verheul H M W
Department of Medical Oncology, Cancer Center Amsterdam, VU University Medical Center, Amsterdam, The Netherlands.
Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands.
Cancer Metastasis Rev. 2017 Jun;36(2):395-406. doi: 10.1007/s10555-017-9668-y.
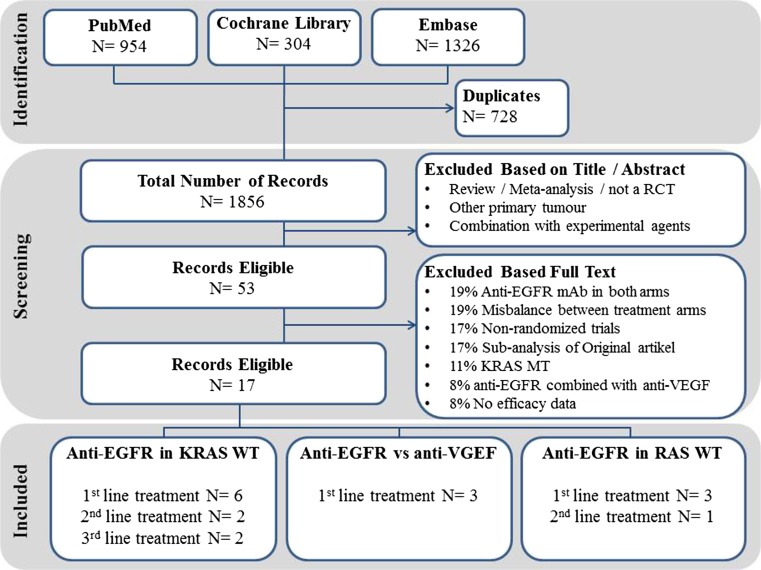
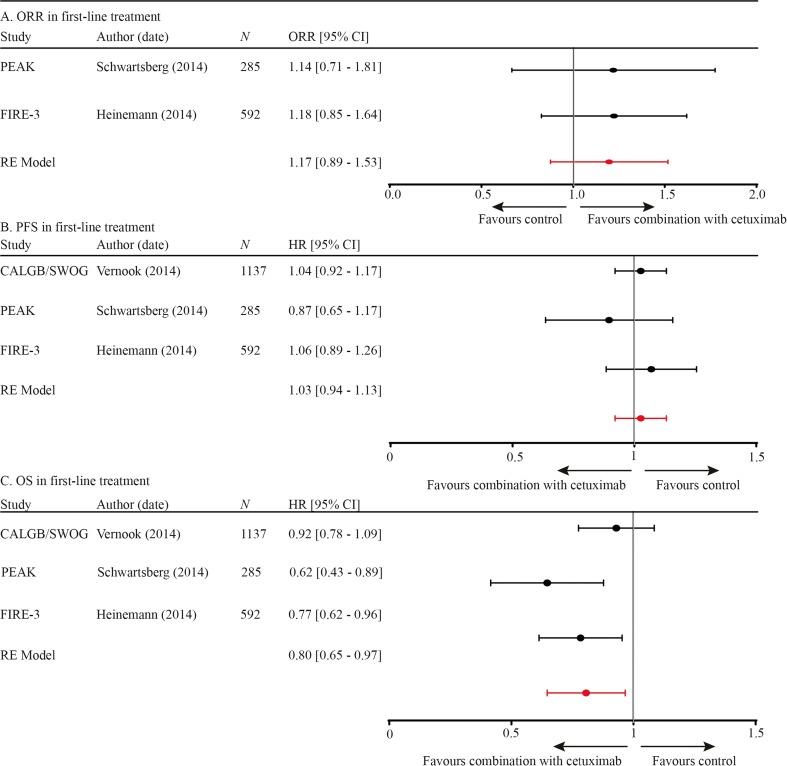
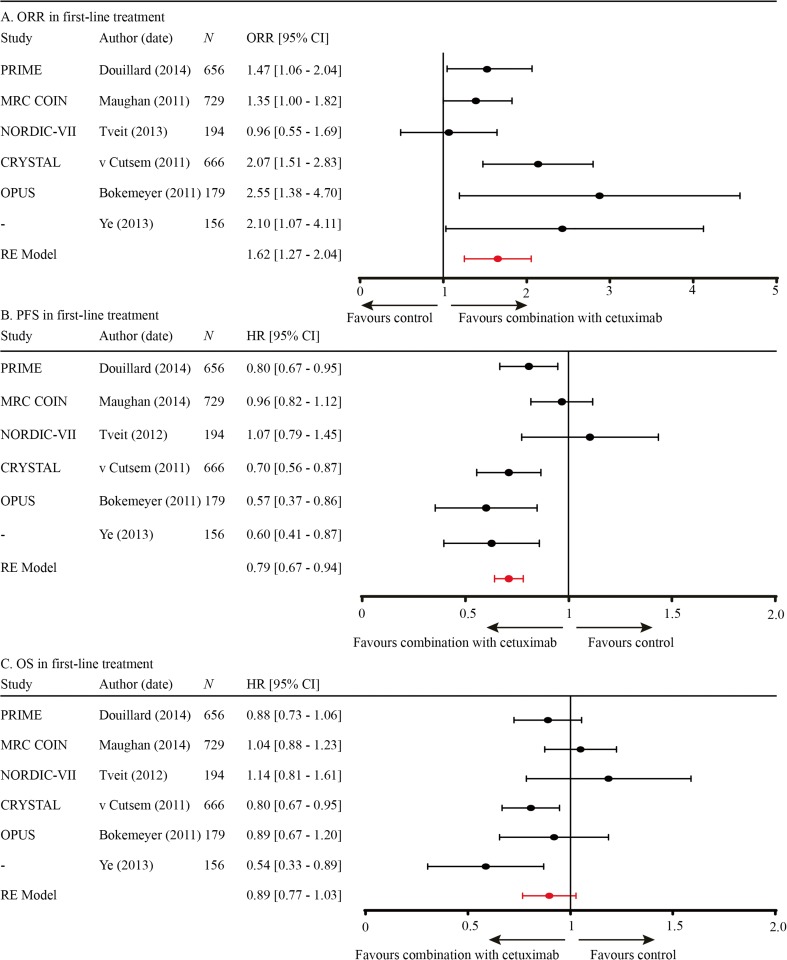
This meta-analysis was performed to determine the optimal use of anti-EGFR mAb in the treatment of metastasized colorectal cancer (mCRC). Seventeen randomized clinical trials were included, all evaluating the added value of anti-EGFR mAb to standard treatment line in patients with KRAS wild-type mCRC. Hazard and odds ratios were pooled using a random effect model, weighted according to cohort size. Pooled data of six first- and two second-line studies demonstrated a significantly improved ORR (OR 1.62, CI 1.27-2.04; OR 4.78, CI 3.39-6.75, respectively) and PFS (HR 0.79, CI 0.67-0.94; HR 0.80, CI 0.71-0.91, respectively) with the addition of anti-EGFR mAb to chemotherapy, while OS remained similar. Two third-line anti-EGFR mAb monotherapy studies revealed an improved PFS and OS (HR 0.44, CI 0.35-0.52; HR 0.55, CI 0.41-0.74). Addition of anti-EGFR versus anti-VEGF mAb to first-line chemotherapy was evaluated in three studies; ORR and PFS were comparable, while OS was improved (HR 0.8, CI 0.65-0.97). The influence of the chemotherapy backbone on anti-EGFR mAb efficacy, evaluated with meta-regression, indicated a higher ORR with irinotecan-based versus oxaliplatin-based regimens, but comparable PFS and OS. Reported toxicity (≥3 grade) increased ~20% in all treatment lines with the addition of anti-EGFR mAb. Anti-EGFR treatment significantly improves response and survival outcome of patients with (K)RAS wild-type mCRC, regardless of treatment line or chemotherapeutic backbone. Saving anti-EGFR mAb as third-line monotherapy is a valid and effective option to prevent high treatment burden caused by combination therapy. Combination treatment with anti-EGFR mAb to achieve radical resection of metastases needs further investigation.
本荟萃分析旨在确定抗表皮生长因子受体(EGFR)单克隆抗体(mAb)在转移性结直肠癌(mCRC)治疗中的最佳应用。纳入了17项随机临床试验,所有试验均评估了抗EGFR mAb在KRAS野生型mCRC患者标准治疗方案基础上的附加价值。采用随机效应模型汇总风险比和优势比,并根据队列规模进行加权。六项一线研究和两项二线研究的汇总数据显示,在化疗基础上加用抗EGFR mAb后,客观缓解率(ORR)显著提高(分别为OR 1.62,CI 1.27 - 2.04;OR 4.78,CI 3.39 - 6.75),无进展生存期(PFS)也显著提高(分别为HR 0.79,CI 0.67 - 0.94;HR 0.80,CI 0.71 - 0.91),而总生存期(OS)保持相似。两项三线抗EGFR mAb单药治疗研究显示PFS和OS有所改善(HR 0.44,CI 0.35 - 0.52;HR 0.55,CI 0.41 - 0.74)。三项研究评估了在一线化疗中加用抗EGFR mAb与抗血管内皮生长因子(VEGF)mAb的情况;ORR和PFS相当,但OS有所改善(HR 0.8,CI 0.65 - 0.97)。通过Meta回归评估化疗方案对抗EGFR mAb疗效的影响,结果表明,与基于奥沙利铂的方案相比,基于伊立替康的方案ORR更高,但PFS和OS相当。在所有治疗线中,加用抗EGFR mAb后报告的毒性(≥3级)增加了约20%。抗EGFR治疗可显著改善(K)RAS野生型mCRC患者的缓解率和生存结局,无论治疗线或化疗方案如何。将抗EGFR mAb留作三线单药治疗是预防联合治疗导致高治疗负担的有效选择。抗EGFR mAb联合治疗以实现转移灶的根治性切除需要进一步研究。