Huang Chih-Chieh, Tsai Kuo-Wang, Tsai Tzung-Jiun, Hsu Ping-I
Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Veterans General Hospital and National Yang-Ming University, Kaohsiung, Taiwan.
Department of Medical Education and Research, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan.
Biomark Res. 2017 Jul 11;5:23. doi: 10.1186/s40364-017-0103-x. eCollection 2017.
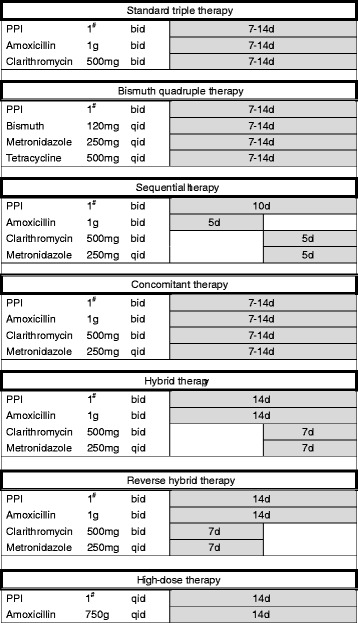
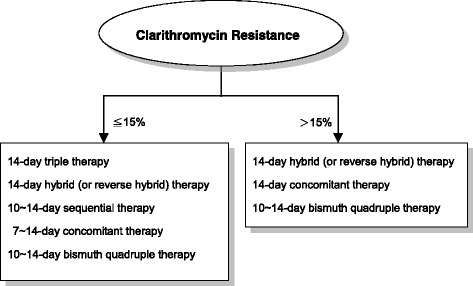
Because the prevalence of antibiotic resistance markedly increases with time worldwide, anti- treatment is continuing to be a great challenge forsphysicians in clinical practice. The Real-world Practice & Expectation of Asia-Pacific Physicians and Patients in Eradication (REAP-HP) Survey demonstrated that the accepted minimal eradication rate of anti- regimen in -infected patients was 91%. The Kyoto Consensus Report on Gastritis also recommended that, within any region, only regimens which reliably produce eradication rates of ≥90% in that population should be used for empirical treatment. This article is aimed to review current first-line eradication regimens with a per-protocol eradication rate exceeding 90% in most geographic areas. In regions with low (≦15%) clarithromycin resistance, 14-day hybrid (or reverse hybrid), 10 ~ 14-day sequential, 7 ~ 14-day concomitant, 10 ~ 14-day bismuth quadruple or 14-day triple therapy can achieve a high eradication rate in the first-line treatment of infection. However, in areas with high (>15%) clarithromycin resistance, standard triple therapy should be abandoned because of low eradication efficacy, and 14-day hybrid (or reverse hybrid), 10 ~ 14-day concomitant or 10 ~ 14-day bismuth quadruple therapy are the recommended regimens. If no recent data of local antibiotic resistances of strains are available, universal high efficacy regimens such as 14-day hybrid (or reverse hybrid), concomitant or bismuth quadruple therapy can be adopted to meet the recommendation of consensus report and patients' expectation.
由于全球范围内抗生素耐药性的患病率随时间显著增加,抗幽门螺杆菌治疗仍然是临床实践中医师面临的巨大挑战。亚太地区医师和患者根除幽门螺杆菌的真实世界实践与期望(REAP-HP)调查显示,幽门螺杆菌感染患者接受的抗幽门螺杆菌方案的最低根除率为91%。《京都胃炎共识报告》也建议,在任何地区,只有在该人群中能可靠产生≥90%根除率的方案才可用于经验性治疗。本文旨在综述目前在大多数地理区域按方案根除率超过90%的一线根除方案。在克拉霉素耐药率低(≤15%)的地区,14天混合(或反向混合)、10至14天序贯、7至14天联合、10至14天铋剂四联或14天三联疗法在幽门螺杆菌感染的一线治疗中可实现高根除率。然而,在克拉霉素耐药率高(>15%)的地区,由于根除疗效低,应放弃标准三联疗法,推荐使用14天混合(或反向混合)、10至14天联合或10至14天铋剂四联疗法。如果没有当地幽门螺杆菌菌株抗生素耐药性的最新数据,可采用14天混合(或反向混合)、联合或铋剂四联疗法等普遍高效方案,以满足共识报告的建议和患者的期望。