Karmali Shamir N, Sciusco Alberto, May Shaun M, Ackland Gareth L
Translational Medicine & Therapeutics, William Harvey Research Institute, Queen Mary University of London, John Vane Science Centre, Charterhouse Square, London, EC1M 6BQ, UK.
Intensive Care Med Exp. 2017 Dec;5(1):33. doi: 10.1186/s40635-017-0146-1. Epub 2017 Jul 12.
Heart rate variability (HRV) has been used to assess cardiac autonomic activity in critically ill patients, driven by translational and biomarker research agendas. Several clinical and technical factors can interfere with the measurement and/or interpretation of HRV. We systematically evaluated how HRV parameters are acquired/processed in critical care medicine.
PubMed, MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (1996-2016) were searched for cohort or case-control clinical studies of adult (>18 years) critically ill patients using heart variability analysis. Duplicate independent review and data abstraction. Study quality was assessed using two independent approaches: Newcastle-Ottowa scale and Downs and Black instrument. Conduct of studies was assessed in three categories: (1) study design and objectives, (2) procedures for measurement, processing and reporting of HRV, and (3) reporting of relevant confounding factors.
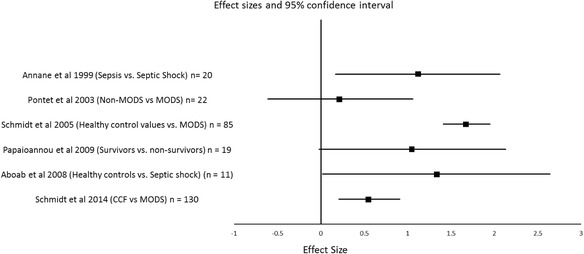
Our search identified 31/271 eligible studies that enrolled 2090 critically ill patients. A minority of studies (15; 48%) reported both frequency and time domain HRV data, with non-normally distributed, wide ranges of values that were indistinguishable from other (non-critically ill) disease states. Significant heterogeneity in HRV measurement protocols was observed between studies; lack of adjustment for various confounders known to affect cardiac autonomic regulation was common. Comparator groups were often omitted (n = 12; 39%). This precluded meaningful meta-analysis.
Marked differences in methodology prevent meaningful comparisons of HRV parameters between studies. A standardised set of consensus criteria relevant to critical care medicine are required to exploit advances in translational autonomic physiology.
受转化医学和生物标志物研究议程的推动,心率变异性(HRV)已被用于评估重症患者的心脏自主神经活动。若干临床和技术因素会干扰HRV的测量和/或解读。我们系统评估了重症医学中HRV参数是如何获取/处理的。
检索PubMed、MEDLINE、EMBASE和Cochrane对照试验中央注册库(1996年至2016年),查找使用心率变异性分析的成年(>18岁)重症患者的队列或病例对照临床研究。进行重复独立评审和数据提取。采用两种独立方法评估研究质量:纽卡斯尔-渥太华量表和唐斯-布莱克工具。从三个类别评估研究开展情况:(1)研究设计和目标,(2)HRV测量、处理和报告程序,以及(3)相关混杂因素的报告。
我们的检索确定了31项/271项符合条件的研究,纳入了2090例重症患者。少数研究(15项;48%)报告了频域和时域HRV数据,其值呈非正态分布,范围广泛,与其他(非重症)疾病状态无法区分。研究之间观察到HRV测量方案存在显著异质性;普遍缺乏对已知影响心脏自主神经调节的各种混杂因素的调整。比较组常常被省略(n = 12;39%)。这使得有意义的荟萃分析无法进行。
方法上的显著差异妨碍了不同研究之间对HRV参数进行有意义的比较。需要一套与重症医学相关的标准化共识标准,以利用转化自主神经生理学的进展。