Jansson Katharina, Dreckmann Karla, Sommer Wiebke, Avsar Murat, Salman Jawad, Siemeni Thierry, Knöfel Ann-Kathrin, Pauksch Linda, Gottlieb Jens, Frühauf Jörg, Werner Martin, Jonigk Danny, Strüber Martin, Haverich Axel, Warnecke Gregor
Division of Cardiac, Thoracic, Transplantation and Vascular Surgery, Hannover Medical School, Hannover, Germany.
The German Centre for Lung Research, Hannover Medical School, Hannover, Germany.
Transplant Direct. 2017 Jun 6;3(7):e170. doi: 10.1097/TXD.0000000000000689. eCollection 2017 Jul.
Preoperative low-dose whole-body irradiation (IRR) with 1.5 and 7 Gy thymic IRR of the recipient, combined with a perioperative donor splenocyte infusion lead to reliable donor specific peripheral tolerance in our allogeneic porcine lung transplantation model. To reduce the toxicity of this preconditioning regime, modifications of the IRR protocol and their impact on allograft survival were assessed.
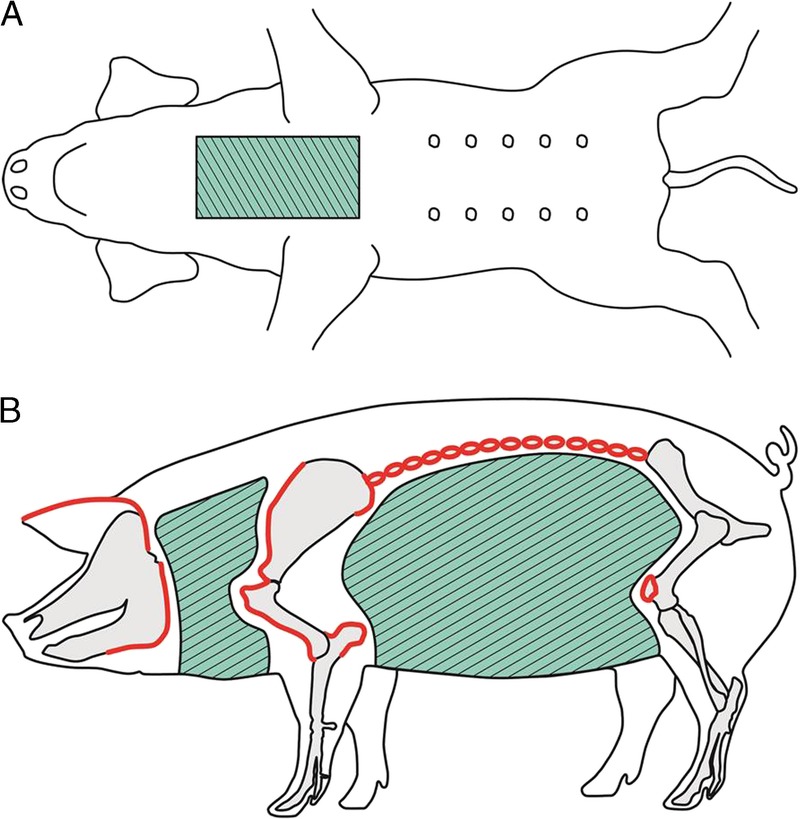
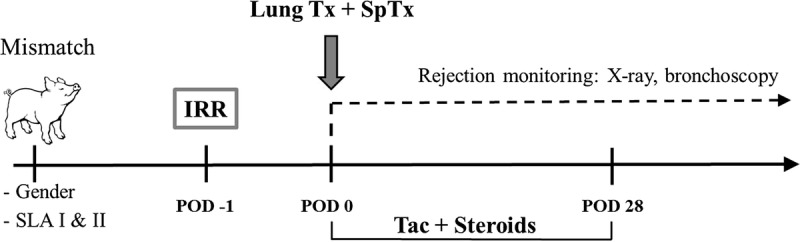
Left-sided single lung transplantation from major histocompatibility complex and sex mismatched donors was performed in 14 adult female minipigs. Recipient animals were exposed to 3 different protocols of nonmyeloablative IRR within 12 hours before transplantation. All animals were administered a donor splenocyte infusion on the day of lung transplantation. Intravenous pharmacologic immunosuppression was withdrawn after 28 postoperative days. Allograft survival was monitored by chest radiographs and bronchoscopy.
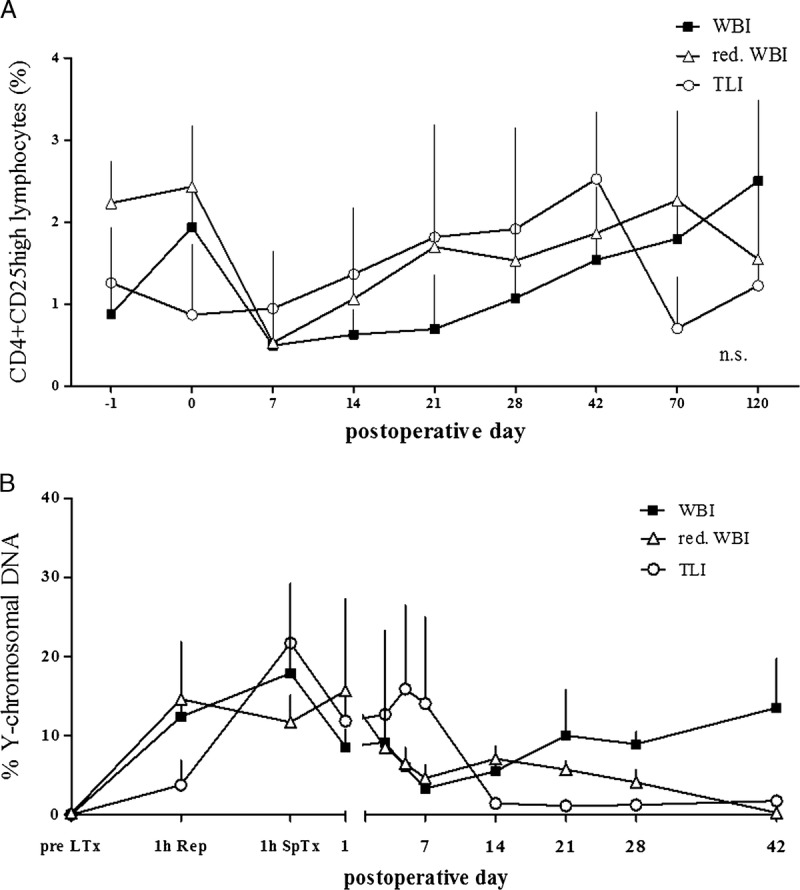
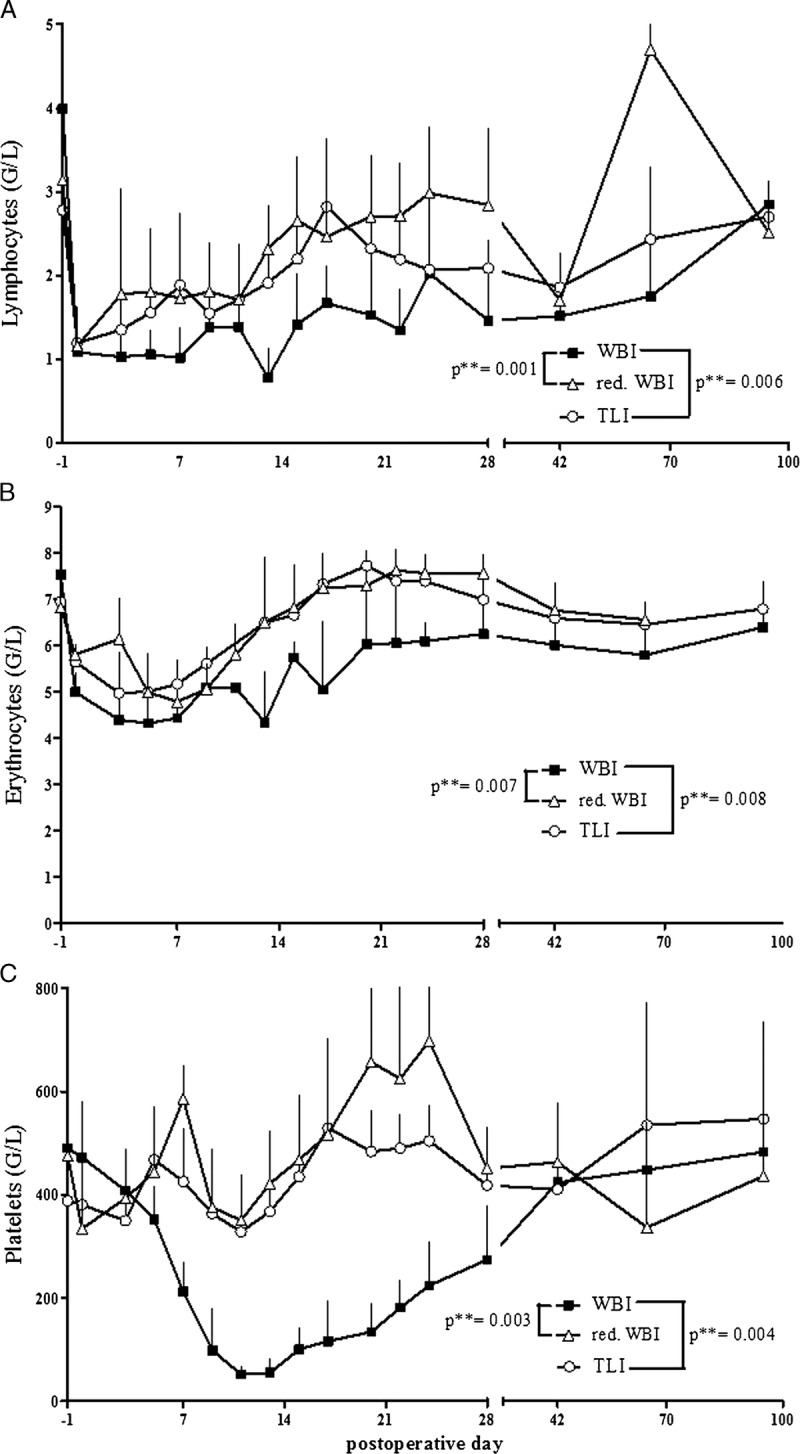
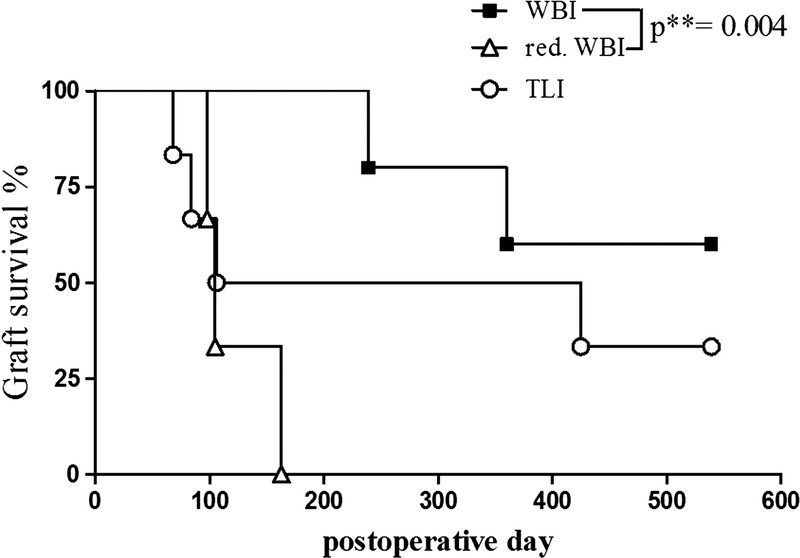
IRR prolonged transplant survival in a dose- and field-dependent manner. Shielding of the bone marrow from IRR (total lymphoid IRR at 1.5 and 7 Gy thymic IRR) significantly reduced protocol toxicity defined as thrombocytopenia and consecutive increased bleeding propensity, but had a less effective impact on graft survival. Whole-body IRR at 0.5 and 7 Gy thymic IRR proved to be ineffective for reliable tolerance induction. Eventually, high levels of circulating CD4CD25 regulatory T cells were present in long-term survivors.
These data show that the infusion of donor-specific alloantigen in combination with IRR is efficient once a threshold dose is exceeded.
在我们的同种异体猪肺移植模型中,术前对受体进行1.5 Gy和7 Gy胸腺照射的低剂量全身照射(IRR),并结合围手术期供体脾细胞输注,可诱导可靠的供体特异性外周耐受。为降低这种预处理方案的毒性,评估了IRR方案的修改及其对同种异体移植存活的影响。
对14只成年雌性小型猪进行了主要组织相容性复合体和性别不匹配供体的左侧单肺移植。受体动物在移植前12小时内接受3种不同的非清髓性IRR方案。所有动物在肺移植当天接受供体脾细胞输注。术后28天停用静脉药物免疫抑制。通过胸部X线片和支气管镜监测同种异体移植存活情况。
IRR以剂量和照射野依赖的方式延长了移植存活时间。对骨髓进行IRR屏蔽(胸腺照射剂量为1.5 Gy和7 Gy时进行全淋巴照射)可显著降低定义为血小板减少和随之增加的出血倾向的方案毒性,但对移植物存活的影响较小。胸腺照射剂量为0.5 Gy和7 Gy时的全身照射被证明对可靠的耐受诱导无效。最终,长期存活者体内存在高水平的循环CD4CD25调节性T细胞。
这些数据表明,一旦超过阈值剂量,供体特异性同种异体抗原输注与IRR联合使用是有效的。