Mahamar Almahamoudou, Issiaka Djibrilla, Barry Amadou, Attaher Oumar, Dembele Adama B, Traore Tiangoua, Sissoko Adama, Keita Sekouba, Diarra Bacary Soumana, Narum David L, Duffy Patrick E, Dicko Alassane, Fried Michal
Malaria Research & Training Center, Faculty of Medicine, Pharmacy and Dentistry, University of Sciences Techniques and Technologies of Bamako, Bamako, Mali.
Laboratory of Malaria Immunology and Vaccinology, NIAID, NIH, 12735 Twinbrook Pkway Building TW3 Room 3W15, Rockville, MD, 20852, USA.
Malar J. 2017 Jul 18;16(1):289. doi: 10.1186/s12936-017-1935-4.
Seasonal malaria chemoprevention (SMC) is a new strategy to reduce malaria burden in young children in Sahelian countries. It consists of the administration of full treatment courses of sulfadoxine-pyrimethamine plus amodiaquine to children at monthly intervals during the malaria season. However, it is not clear if there is a cumulative effect of SMC over time on acquisition of antibodies to malaria antigens.
A cross-sectional serosurvey was carried out 1 month after the last dose of SMC in 2016. Children aged 3-4 years were randomly selected from areas where SMC was given for 1, 2 or 3 years during the malaria season. Children in the areas where SMC had been implemented for 1 year but who failed to receive SMC were used as comparison group. Antibody extracted from dry blood spots was used to measure IgG levels to CSP, MSP-1 and AMA1.
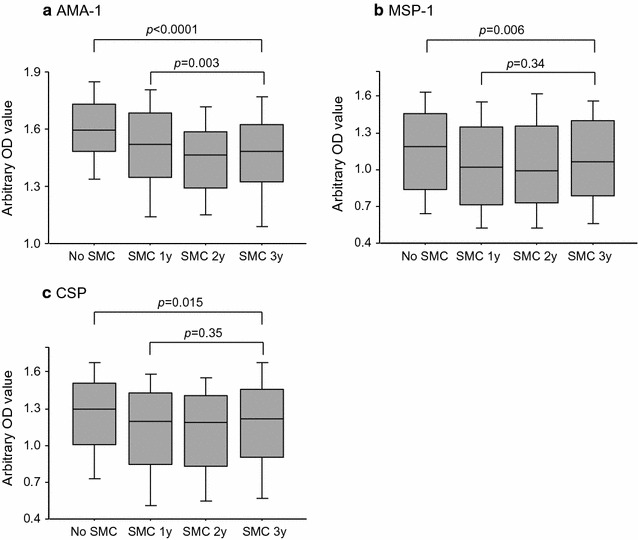
The prevalence of antibodies to AMA-1 were high and similar in children who received SMC for 1, 2 or 3 years and also when compared to those who never received SMC (96.3 vs 97.5%, adjusted OR = 0.99, 95% CI 0.33-2.97, p = 0.99). The prevalence of antibodies to MSP-1 and to CSP were similar in children that received SMC for 1, 2 or 3 years, but were lower in these children compared to those who did not receive SMC (87.1 vs 91.2%, adjusted OR = 0.55, 95% CI 0.29-1.01, p = 0.05 for MSP-1; 79.8 vs 89.2%, adjusted OR = 0.52, 95% CI 0.30-0.90, p = 0.019 for CSP).
SMC reduced seropositivity to MSP-1 and CSP, but the duration of SMC did not further reduce seropositivity. Exposure to SMC did not reduce the seropositivity to AMA1.
季节性疟疾化学预防(SMC)是一项旨在减轻萨赫勒地区国家幼儿疟疾负担的新策略。它包括在疟疾季节每月为儿童提供磺胺多辛-乙胺嘧啶加阿莫地喹的完整疗程。然而,目前尚不清楚SMC随着时间的推移对疟疾抗原抗体的获得是否存在累积效应。
在2016年最后一剂SMC给药1个月后进行了一项横断面血清学调查。从疟疾季节接受1、2或3年SMC的地区随机选取3-4岁的儿童。将在已实施SMC 1年但未接受SMC的地区的儿童作为对照组。从干血斑中提取的抗体用于测量针对环子孢子蛋白(CSP)、裂殖子表面蛋白1(MSP-1)和裂殖体表面抗原1(AMA1)的IgG水平。
接受1、2或3年SMC的儿童以及与从未接受SMC的儿童相比,AMA-1抗体的阳性率较高且相似(96.3%对97.5%,校正比值比=0.99,95%置信区间0.33-2.97,p=0.99)。接受1、2或3年SMC的儿童中,MSP-1和CSP抗体的阳性率相似,但与未接受SMC的儿童相比,这些儿童的阳性率较低(MSP-1为87.1%对91.2%,校正比值比=0.55,95%置信区间0.29-1.01,p=0.05;CSP为79.8%对89.2%,校正比值比=0.52,95%置信区间0.30-0.90,p=0.019)。
SMC降低了对MSP-1和CSP的血清阳性率,但SMC的持续时间并未进一步降低血清阳性率。接触SMC并未降低对AMA1的血清阳性率。