Yao James C, Chan Jennifer A, Mita Alain C, Kundu Madan G, Hermosillo Reséndiz Karina, Hu Ke, Ravichandran Shoba, Strosberg Jonathan R, Wolin Edward M
GI Medical Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX.
Gastrointestinal Cancer Center, Dana-Farber Cancer Institute, Boston, MA.
Onco Targets Ther. 2017 Jun 27;10:3177-3186. doi: 10.2147/OTT.S128547. eCollection 2017.
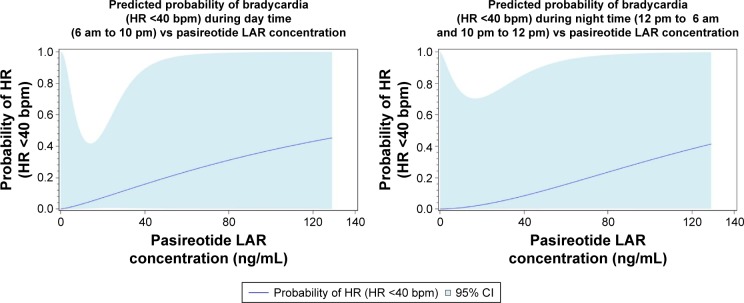
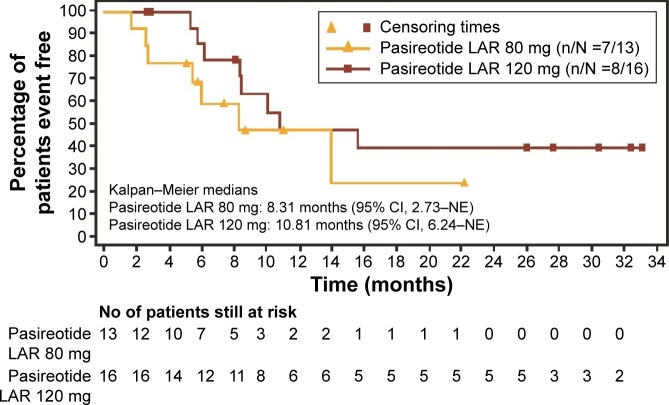
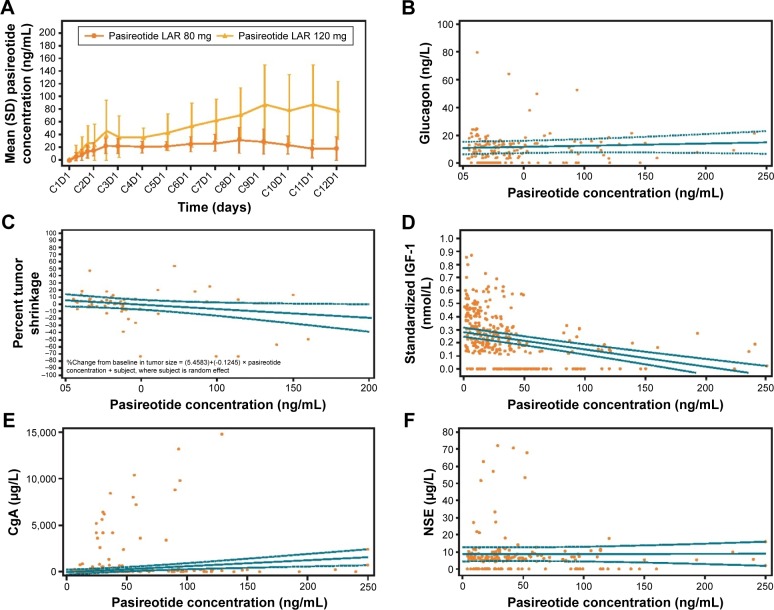
This phase I study aimed at determining the maximum tolerated dose (MTD) and characterizing the safety, tolerability, pharmacokinetics (PKs), and efficacy of pasireotide in patients with advanced neuroendocrine tumors (NETs). Patients were enrolled in two phases: dose-escalation phase (to determine the MTD) at a starting dose of 80 mg pasireotide long-acting release (LAR) i.m. followed by a dose-expansion phase (to evaluate safety and prelimi-nary efficacy). Associations between PK/pharmacodynamic parameters and clinical outcomes were evaluated using linear regression analysis. A total of 29 patients were treated with 80 mg (n=13) and 120 mg (n=16) doses. Most common primary tumor sites included small intestine (44.8%), pancreas (24.1%), and lung (17.2%). No protocol-defined dose-limiting toxicities were observed in the study; however, in post hoc analysis, a higher incidence of bradycardia (heart rate [HR] <40 beats per minute [bpm]) was observed with 120 mg (31.3%) vs 80 mg (0%). Two partial responses (PRs) were observed, both in the 120 mg dose cohort. Pasireotide concentrations correlated with tumor shrinkage, although the association was not statistically significant (=0.08). Among the biomarkers analyzed, insulin-like growth factor 1 (IGF-1) showed a decreasing trend with increasing pasireotide concentration, while chromogranin A (CgA) and neuron-specific enolase (NSE) levels did not show any dose-response relationship. The most common adverse events in any dose group were hyperglycemia, fatigue, and nausea. MTD was defined at 120 mg for pasireotide LAR in patients with advanced NETs. Although objective radiographic responses were rarely observed with somatostatin analogs, two PRs were observed among 16 patients in the 120 mg cohort. Bradycardia (HR <40 bpm) appears to be a dose-limiting effect; however, the mechanism and clinical significance are uncertain. This study was registered with clinicaltrials.gov (NCT01364415).
这项I期研究旨在确定最大耐受剂量(MTD),并对帕西瑞肽在晚期神经内分泌肿瘤(NET)患者中的安全性、耐受性、药代动力学(PK)和疗效进行特征描述。患者分为两个阶段入组:剂量递增阶段(确定MTD),起始剂量为帕西瑞肽长效释放(LAR)80mg,肌肉注射,随后是剂量扩展阶段(评估安全性和初步疗效)。使用线性回归分析评估PK/药效学参数与临床结果之间的关联。共有29例患者接受了80mg(n = 13)和120mg(n = 16)剂量的治疗。最常见的原发肿瘤部位包括小肠(44.8%)、胰腺(24.1%)和肺(17.2%)。研究中未观察到方案定义的剂量限制性毒性;然而,在事后分析中,120mg组(31.3%)与80mg组(0%)相比,心动过缓(心率[HR]<40次/分钟[bpm])的发生率更高。观察到两例部分缓解(PR),均在120mg剂量队列中。帕西瑞肽浓度与肿瘤缩小相关,尽管这种关联无统计学意义(=0.08)。在分析的生物标志物中,胰岛素样生长因子1(IGF-1)随帕西瑞肽浓度升高呈下降趋势,而嗜铬粒蛋白A(CgA)和神经元特异性烯醇化酶(NSE)水平未显示任何剂量反应关系。任何剂量组中最常见的不良事件为高血糖、疲劳和恶心。晚期NET患者中帕西瑞肽LAR的MTD定义为120mg。尽管使用生长抑素类似物很少观察到客观的影像学反应,但在120mg队列的16例患者中观察到两例PR。心动过缓(HR<40bpm)似乎是一种剂量限制性效应;然而,其机制和临床意义尚不确定。本研究已在clinicaltrials.gov注册(NCT01364415)。