de Jonge Stijn Willem, Gans Sarah L, Atema Jasper J, Solomkin Joseph S, Dellinger Patchen E, Boermeester Marja A
Department of Surgery, Academic Medical Center, Amsterdam, The Netherlands Department of Surgery, University of Cincinnati College of Medicine, Cincinnati, OH Department of Surgery, University of Washington Medical Center, Washington, DC.
Medicine (Baltimore). 2017 Jul;96(29):e6903. doi: 10.1097/MD.0000000000006903.
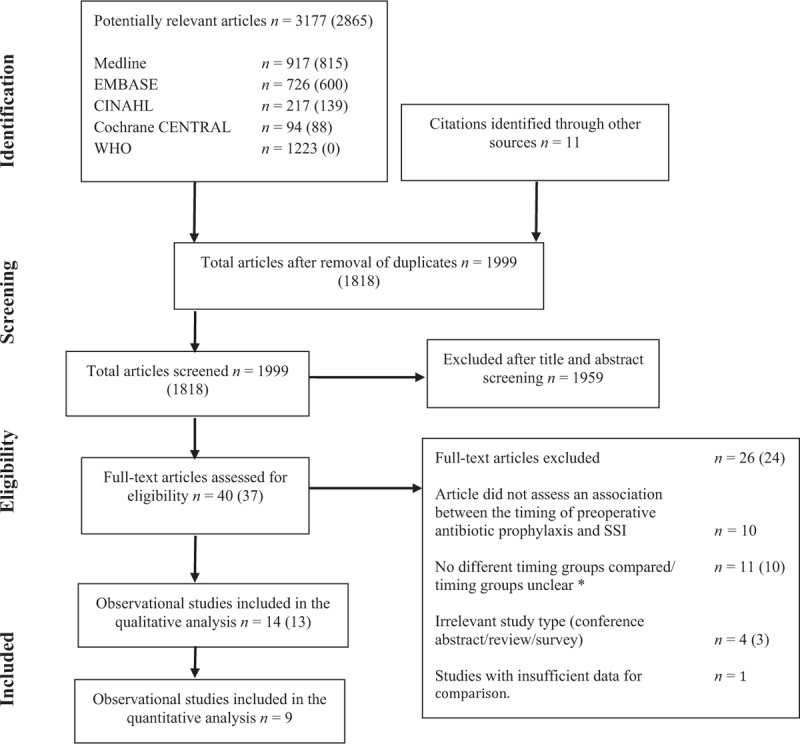
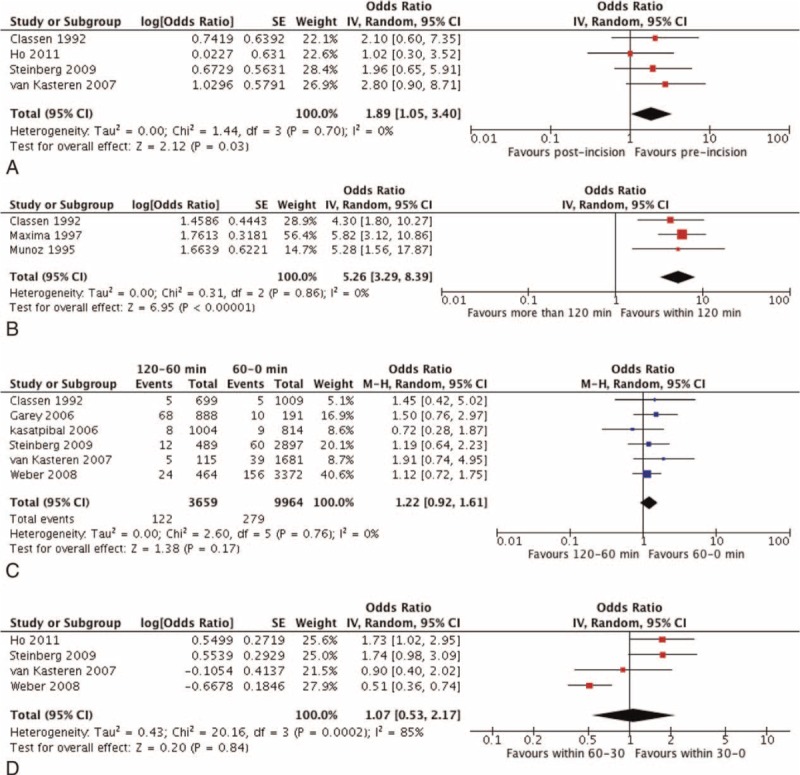
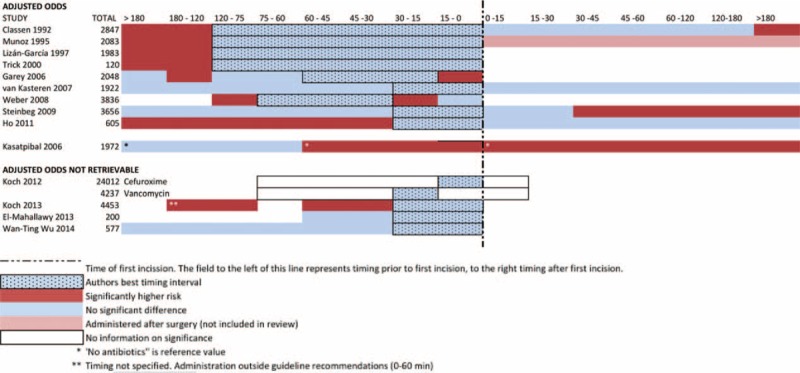
The aim of the study was to assess the effect of timing of preoperative surgical antibiotic prophylaxis (SAP) on surgical site infection (SSI) and compare the different timing intervals.The benefit of routine use of SAP prior to surgery has long been recognized. However, the optimal timing has not been defined. For the purpose of developing recommendations for the World Health Organization guideline for SSI prevention, a systematic review and meta-analysis of all relevant evidence was conducted.Major medical databases were searched from 1990 to 2016. The primary outcome was SSI after preoperative-SAP comparing different timing intervals. Adjusted odds ratios (OR) with 95% confidence intervals (CI) were extracted and pooled for each comparison with a random effects model.Fourteen papers with 54,552 patients were included in this review. In a quantitative analysis, there was no significant difference when SAP was administered 120-60 minutes prior to incision compared to administration 60-0 minutes prior to incision. Studies investigating different timing intervals within the last 60 minutes time frame reported contradictive results. The risk of SSI almost doubled when SAP was administered after first incision (OR:1.89; 95%CI:[1.05-3.40]) and was 5 times higher when administered more than 120 minutes prior to incision (OR5.26; 95%CI:[3.29-8.39]).Administration of antibiotic prophylaxis more than 120 minutes before incision or after incision is associated a higher risk of surgical site infections than administration less than 120 minutes before incision. Within this 120-minute time frame prior to incision, no differential effects could be identified. The broadly accepted recommendation to administer prophylaxis within a 60-minute time frame prior to incision could not be substantiated.
本研究的目的是评估术前手术预防性抗生素(SAP)给药时机对手术部位感染(SSI)的影响,并比较不同的时间间隔。术前常规使用SAP的益处早已得到认可。然而,最佳给药时机尚未确定。为了制定世界卫生组织预防SSI指南的建议,我们对所有相关证据进行了系统评价和荟萃分析。检索了1990年至2016年的主要医学数据库。主要结局是术前SAP后不同时间间隔比较的SSI。提取并合并每个比较的调整比值比(OR)及其95%置信区间(CI),采用随机效应模型。本评价纳入了14篇文献,共54552例患者。在定量分析中,术前120 - 60分钟给药与术前60 - 0分钟给药相比,差异无统计学意义。在最后60分钟时间范围内研究不同时间间隔的研究报告了相互矛盾的结果。首次切口后给予SAP时,SSI风险几乎增加一倍(OR:1.89;95%CI:[1.05 - 3.40]),术前超过120分钟给药时,SSI风险则高出5倍(OR 5.26;95%CI:[3.29 - 8.39])。术前超过120分钟或术后给予预防性抗生素与术前少于120分钟给药相比,手术部位感染风险更高。在切口前120分钟的时间范围内,未发现差异效应。术前60分钟内给药这一广泛接受的建议无法得到证实。