Nishida Takeshi, Kinoshita Takahiro, Yamakawa Kazuma
Division of Trauma and Surgical Critical Care, Osaka General Medical Center, 3-1-56 Bandai-Higashi, Sumiyoshi-ku, Osaka, 558-8558 Japan.
J Intensive Care. 2017 Jan 20;5:5. doi: 10.1186/s40560-016-0201-0. eCollection 2017.
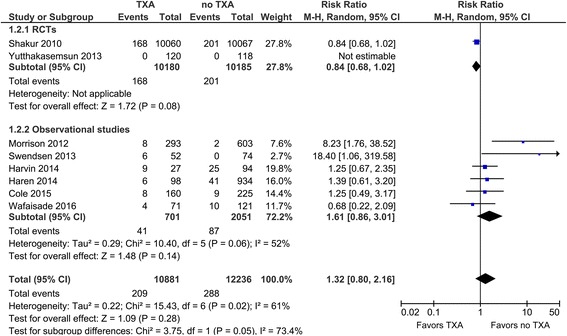
Tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine that inhibits fibrinolysis by blocking the interaction of plasminogen with the lysine residues of fibrin. Historically, TXA is commonly used for reduction of blood loss in perioperative situations, while recently it has attracted attention for clinical use in the trauma field. In 2010, the Clinical Randomization of an Antifibrinolytic in Significant Hemorrhage 2 (CRASH-2) trial demonstrated that intravenous administration of TXA improved mortality significantly in trauma patients with significant bleeding. After the launch of its sensational results, the main stream treatment protocol in trauma changed worldwide to include TXA administration. In this review, first we summarize the recent evidence or recommendations in the related guidelines concerning TXA. Also, we next tried to explore in detail not only the benefits but also the harm introduced by TXA in trauma patients, because the main adverse event results for TXA, such as vascular occlusive events in the CRASH-2 trial, are still being discussed in several papers. Thus, we briefly summarized the evidence for the safety of TXA administration by a systematic review method using observational studies. Consequently, the pooled relative risk for venous thromboembolisms was 1.61 (95% CI, 0.86-3.01), indicating a non-significant increase in the venous thromboembolism risk of TXA therapy. Regarding the basic mechanism, TXA potentially possesses the risk of venous thromboembolisms, so it should be used cautiously and selectively. Further investigation is needed to delineate the optimal targeted trauma patients to earn the maximum survival benefits with minimized risk of thrombotic complications.
氨甲环酸(TXA)是氨基酸赖氨酸的合成衍生物,它通过阻断纤溶酶原与纤维蛋白赖氨酸残基的相互作用来抑制纤维蛋白溶解。从历史上看,TXA常用于减少围手术期的失血,而最近它在创伤领域的临床应用引起了关注。2010年,重大出血中抗纤溶药物的临床随机试验2(CRASH-2)表明,静脉注射TXA可显著提高严重出血创伤患者的生存率。在其惊人结果公布后,全球创伤的主流治疗方案改变为包括使用TXA。在本综述中,首先我们总结了相关指南中关于TXA的最新证据或建议。此外,接下来我们不仅试图详细探讨TXA给创伤患者带来的益处,还探讨其危害,因为关于TXA的主要不良事件结果,如CRASH-2试验中的血管闭塞事件,仍在多篇论文中讨论。因此,我们通过使用观察性研究的系统评价方法简要总结了TXA给药安全性的证据。结果显示,静脉血栓栓塞的合并相对风险为1.61(95%CI,0.86 - 3.01),表明TXA治疗的静脉血栓栓塞风险无显著增加。就基本机制而言,TXA潜在地具有静脉血栓栓塞的风险,因此应谨慎且有选择地使用。需要进一步研究以确定最佳的目标创伤患者,从而在使血栓形成并发症风险最小化的同时获得最大的生存益处。