Eronia Nilde, Mauri Tommaso, Maffezzini Elisabetta, Gatti Stefano, Bronco Alfio, Alban Laura, Binda Filippo, Sasso Tommaso, Marenghi Cristina, Grasselli Giacomo, Foti Giuseppe, Pesenti Antonio, Bellani Giacomo
Department of Emergency and Intensive Care, San Gerardo Hospital, Via Pergolesi 33, Monza, Italy.
Department of Pathophysiology and Transplantation, University of Milan, Via Festa del Perdono 7, Milan, Italy.
Ann Intensive Care. 2017 Dec;7(1):76. doi: 10.1186/s13613-017-0299-9. Epub 2017 Jul 20.
Positive end-expiratory pressure (PEEP) is a key element of mechanical ventilation. It should optimize recruitment, without causing excessive overdistension, but controversy exists on the best method to set it. The purpose of the study was to test the feasibility of setting PEEP with electrical impedance tomography in order to prevent lung de-recruitment following a recruitment maneuver. We enrolled 16 patients undergoing mechanical ventilation with PaO/FiO <300 mmHg. In all patients, under constant tidal volume (6-8 ml/kg) PEEP was set based on the PEEP/FiO table proposed by the ARDS network (PEEP). We performed a recruitment maneuver and monitored the end-expiratory lung impedance (EELI) over 10 min. If the EELI signal decreased during this period, the recruitment maneuver was repeated and PEEP increased by 2 cmHO. This procedure was repeated until the EELI maintained a stability over time (PEEP).
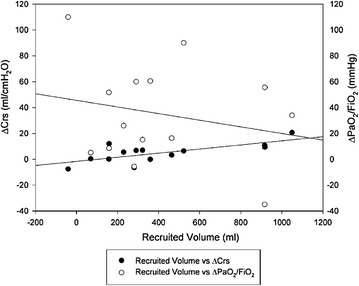
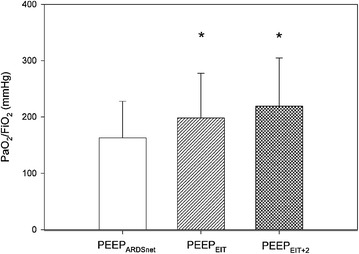
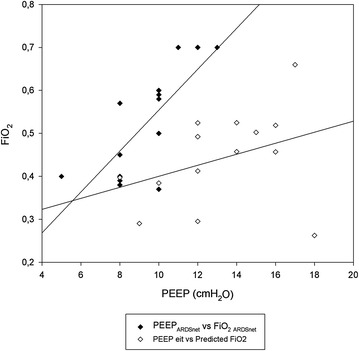
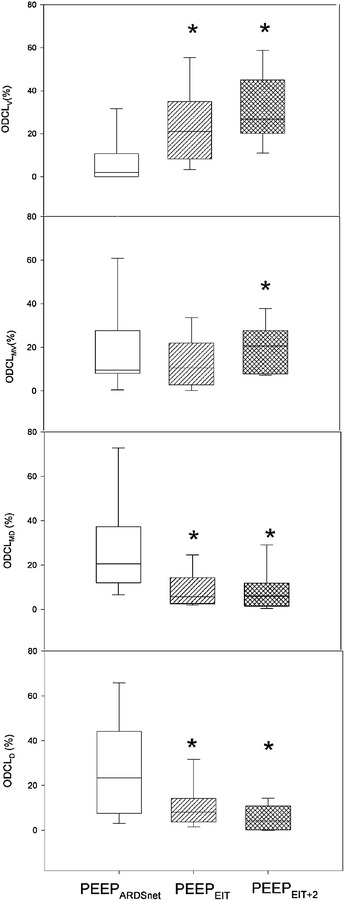
The procedure was feasible in 87% patients. PEEP was higher than PEEP (13 ± 3 vs. 9 ± 2 cmHO, p < 0.001). PaO/FiO improved during PEEP and driving pressure decreased. Recruited volume correlated with the decrease in driving pressure but not with oxygenation improvement. Finally, regional alveolar hyperdistention and collapse was reduced in dependent lung layers and increased in non-dependent lung layers.
In hypoxemic patients, a PEEP selection strategy aimed at stabilizing alveolar recruitment guided by EIT at the bedside was feasible and safe. This strategy led, in comparison with the ARDSnet table, to higher PEEP, improved oxygenation and reduced driving pressure, allowing to estimate the relative weight of overdistension and recruitment.
呼气末正压(PEEP)是机械通气的关键要素。它应优化肺复张,而不引起过度膨胀,但关于设置PEEP的最佳方法仍存在争议。本研究的目的是测试使用电阻抗断层扫描设置PEEP以防止肺复张后肺再萎陷的可行性。我们纳入了16例机械通气且氧合指数(PaO₂/FiO₂)<300 mmHg的患者。在所有患者中,在恒定潮气量(6 - 8 ml/kg)下,根据急性呼吸窘迫综合征(ARDS)网络推荐的PEEP/FiO₂表格设置PEEP(PEEP₁)。我们进行了肺复张操作,并在10分钟内监测呼气末肺阻抗(EELI)。如果在此期间EELI信号下降,则重复肺复张操作并将PEEP增加2 cmH₂O。重复此过程,直到EELI随时间保持稳定(PEEP₂)。
该操作在87%的患者中可行。PEEP₂高于PEEP₁(13 ± 3 vs. 9 ± 2 cmH₂O,p < 0.001)。在PEEP₂期间氧合指数改善,驱动压降低。复张容积与驱动压的降低相关,但与氧合改善无关。最后,在重力依赖肺区,局部肺泡过度膨胀和萎陷减少,而非重力依赖肺区增加。
在低氧血症患者中,一种在床旁通过电阻抗断层扫描引导以稳定肺泡复张为目标的PEEP选择策略是可行且安全的。与ARDS网络表格相比,该策略导致更高的PEEP、改善的氧合和降低的驱动压,从而能够评估过度膨胀和复张的相对权重。