McDonnell Sharon L, Baggerly Keith A, Baggerly Carole A, Aliano Jennifer L, French Christine B, Baggerly Leo L, Ebeling Myla D, Rittenberg Charles S, Goodier Christopher G, Mateus Niño Julio F, Wineland Rebecca J, Newman Roger B, Hollis Bruce W, Wagner Carol L
GrassrootsHealth, Encinitas, California, United States of America.
Deptartment of Bioinformatics and Computational Biology, The University of Texas MD Anderson Cancer Center, Houston, Texas, United States of America.
PLoS One. 2017 Jul 24;12(7):e0180483. doi: 10.1371/journal.pone.0180483. eCollection 2017.
Given the high rate of preterm birth (PTB) nationwide and data from RCTs demonstrating risk reduction with vitamin D supplementation, the Medical University of South Carolina (MUSC) implemented a new standard of care for pregnant women to receive vitamin D testing and supplementation.
To determine if the reported inverse relationship between maternal 25(OH)D and PTB risk could be replicated at MUSC, an urban medical center treating a large, diverse population.
Medical record data were obtained for pregnant patients aged 18-45 years between September 2015 and December 2016. During this time, a protocol that included 25(OH)D testing at first prenatal visit with recommended follow-up testing was initiated. Free vitamin D supplements were offered and the treatment goal was ≥40 ng/mL. PTB rates (<37 weeks) were calculated, and logistic regression and locally weighted regression (LOESS) were used to explore the association between 25(OH)D and PTB. Subgroup analyses were also conducted.
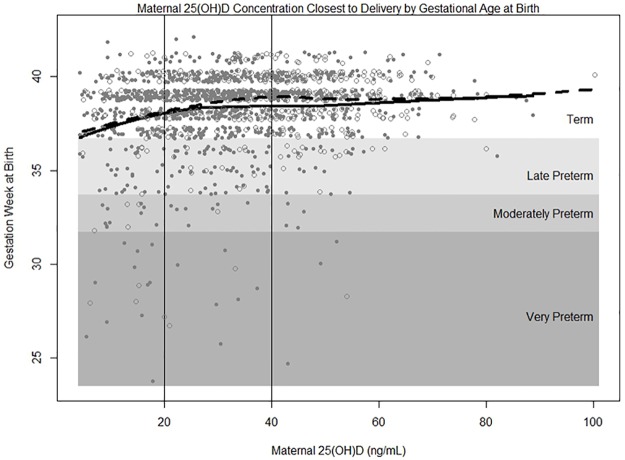
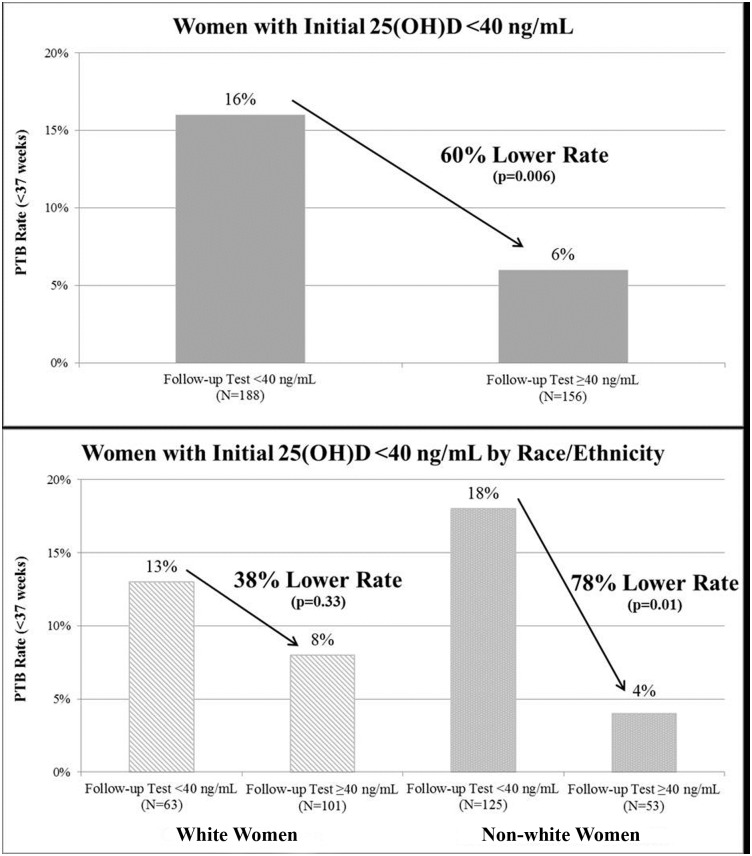
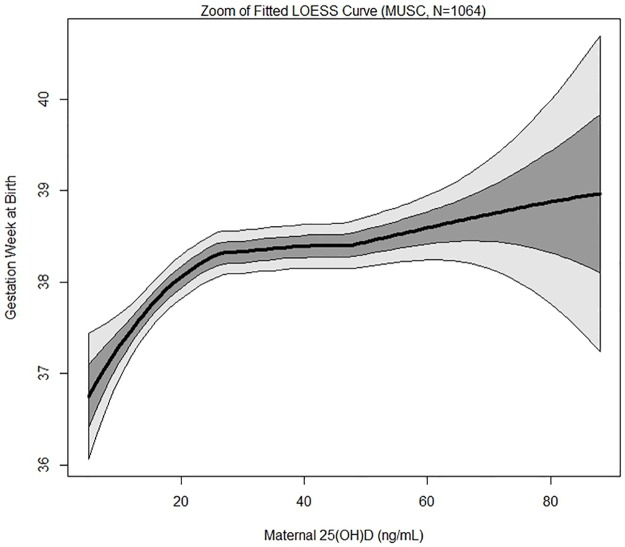
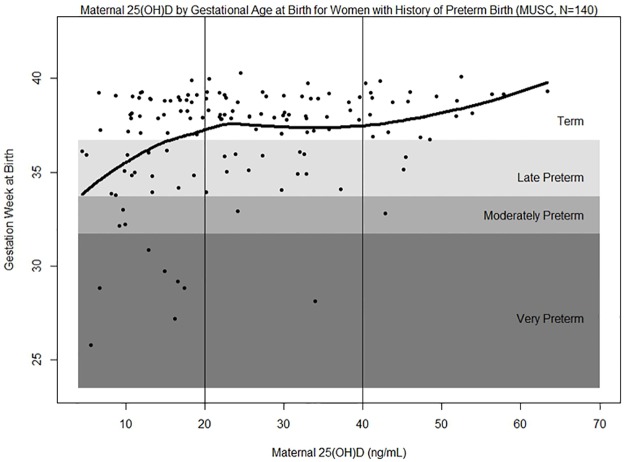
Among women with a live, singleton birth and at least one 25(OH)D test during pregnancy (N = 1,064), the overall PTB rate was 13%. The LOESS curve showed gestational age rising with increasing 25(OH)D. Women with 25(OH)D ≥40 ng/mL had a 62% lower risk of PTB compared to those <20 ng/mL (p<0.0001). After adjusting for socioeconomic variables, this lower risk remained (OR = 0.41, p = 0.002). Similar decreases in PTB risk were observed for PTB subtypes (spontaneous: 58%, p = 0.02; indicated: 61%, p = 0.006), by race/ethnicity (white: 65%, p = 0.03; non-white: 68%, p = 0.008), and among women with a prior PTB (80%, p = 0.02). Among women with initial 25(OH)D <40 ng/mL, PTB rates were 60% lower for those with ≥40 vs. <40 ng/mL on a follow-up test (p = 0.006); 38% for whites (p = 0.33) and 78% for non-whites (p = 0.01).
Maternal 25(OH)D concentrations ≥40 ng/mL were associated with substantial reduction in PTB risk in a large, diverse population of women.
鉴于全国早产(PTB)发生率较高,且随机对照试验(RCT)数据表明补充维生素D可降低风险,南卡罗来纳医科大学(MUSC)实施了一项针对孕妇的新护理标准,即进行维生素D检测和补充。
确定在MUSC(一家治疗大量不同人群的城市医疗中心)是否能重现所报道的母体25(OH)D与PTB风险之间的负相关关系。
获取了2015年9月至2016年12月期间年龄在18 - 45岁的孕妇的病历数据。在此期间,启动了一项方案,包括首次产前检查时进行25(OH)D检测及建议的后续检测。提供免费维生素D补充剂,治疗目标是≥40 ng/mL。计算早产(<37周)发生率,并使用逻辑回归和局部加权回归(LOESS)来探讨25(OH)D与PTB之间的关联。还进行了亚组分析。
在有活产单胎且孕期至少进行过一次25(OH)D检测的女性中(N = 1064),总体早产率为13%。LOESS曲线显示孕周随25(OH)D升高而增加。25(OH)D≥40 ng/mL的女性与<20 ng/mL的女性相比,早产风险降低62%(p<0.0001)。在调整社会经济变量后,这种较低风险仍然存在(比值比 = 0.41,p = 0.002)。在早产亚型(自发早产:58%,p = 0.02;医源性早产:61%,p = 0.006)、按种族/族裔(白人:65%,p = 0.03;非白人:68%,p = 0.008)以及有既往早产史的女性中(80%,p = 0.02),均观察到类似的早产风险降低情况。在初始25(OH)D<40 ng/mL的女性中,后续检测时25(OH)D≥40 ng/mL的女性与<40 ng/mL的女性相比,早产率降低60%(p = 0.006);白人降低38%(p = 0.33),非白人降低78%(p = 0.01)。
母体25(OH)D浓度≥40 ng/mL与大量不同女性人群的早产风险显著降低相关。