Sakata Taizo, Katagiri Hideki, Kubota Tadao, Sakamoto Takashi, Yoshikawa Kentaro, Lefor Alan Kawarai, Jung Cheol Woong, Kojima Toru
Department of Surgery, Okayama Saiseikai General Hospital, Okayama, Japan.
Department of Surgery, Tokyo Bay Urayasu Ichikawa Medical Center, Chiba, Japan.
Int J Surg Case Rep. 2017;38:69-72. doi: 10.1016/j.ijscr.2017.07.016. Epub 2017 Jul 14.
Pancreas transplantation is the best treatment option in selected patients with type 1 diabetes mellitus. Here we report a patient with a nonmarginal duodenal perforation five years after a simultaneous pancreas-living donor kidney transplantation (SPLKT).
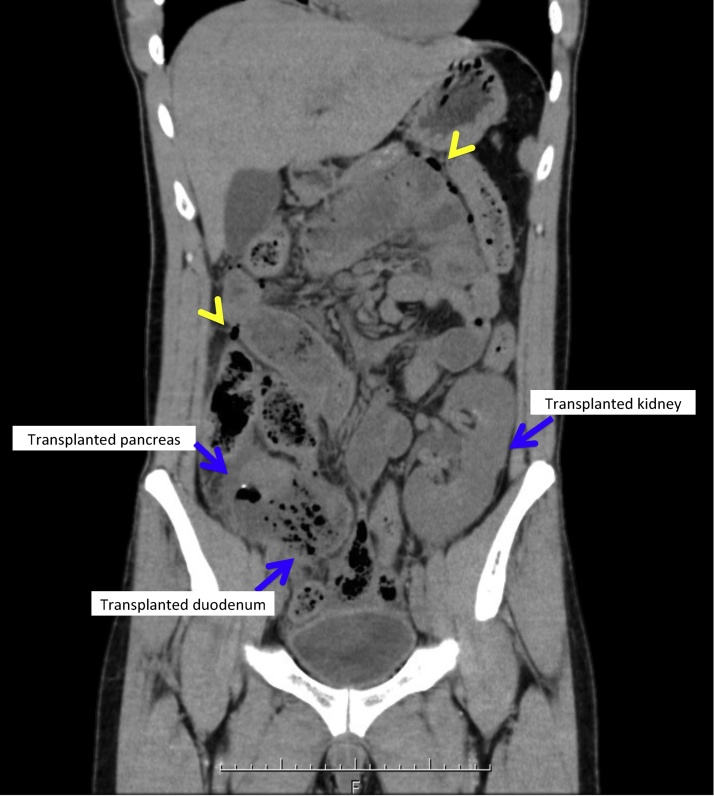
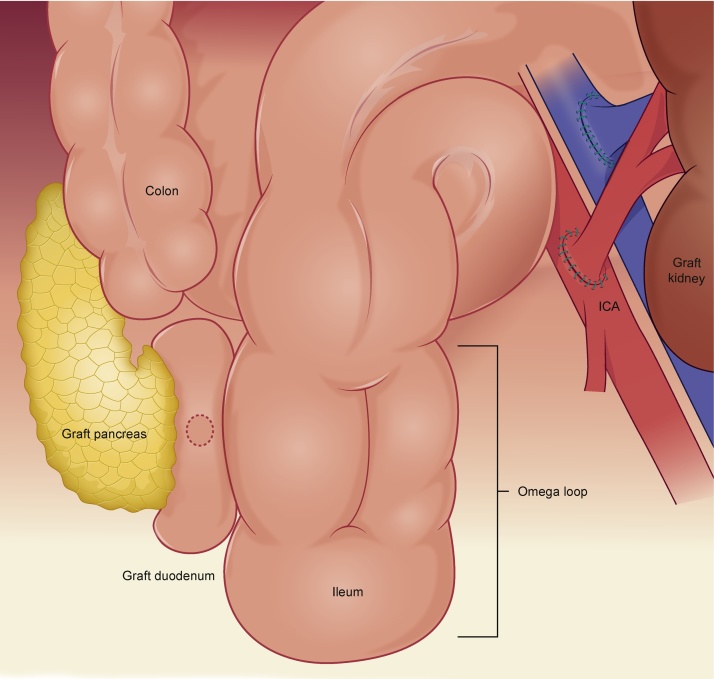
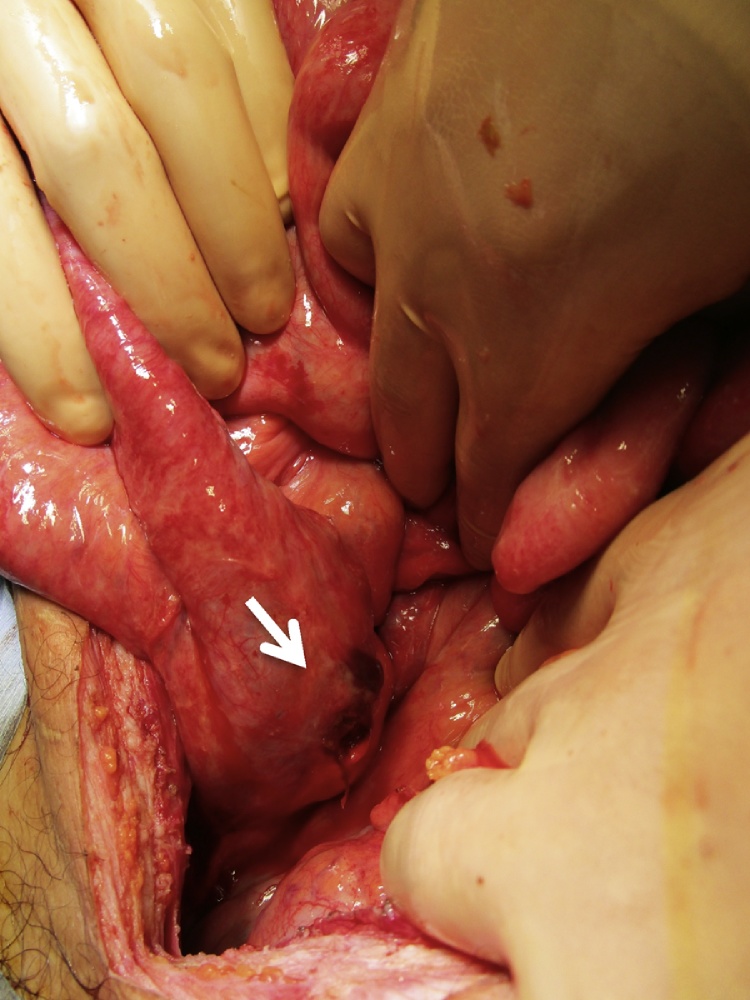
A 31-year old male who underwent SPLKT five years previously presented with severe abdominal pain. He had a marginal duodenal perforation four years later, treated by primary closure and drainage. Biopsy of the pancreas and duodenum graft at that time showed chronic rejection in the pancreas and acute inflammation with an ulcer in the duodenum. At presentation, computerized tomography scan showed mesenteric pneumatosis with enteric leak and ileal dilatation proximal to the anastomotic site. We performed emergent laparotomy and found a 1.0cm perforation at the nonmarginal, posterior wall of the duodenum. Undigested fiber-rich food was extracted from the site and an omental patch placed over the perforation. An ileostomy was created proximal to the omega loop for decompression and a drain placed nearby. The postoperative course was unremarkable.
There are only eight previous cases of graft duodenal perforation in the literature. Fiber-rich food residue passing through the anastomosis with impaction may have led to this perforation.
When a patient is stable, even in the presence of delayed duodenal graft perforation, graft excision may not be necessary. Intraoperative exploration should include Doppler ultrasound examination of the vasculature to rule out thrombosis as a contributor to ischemia. Tissue biopsy should be performed to diagnose rejection.
胰腺移植是特定1型糖尿病患者的最佳治疗选择。在此,我们报告一例在同时进行胰腺-活体供肾移植(SPLKT)五年后发生非边缘性十二指肠穿孔的患者。
一名31岁男性,五年前接受了SPLKT,现出现严重腹痛。四年后他发生了边缘性十二指肠穿孔,接受了一期缝合和引流治疗。当时对胰腺和十二指肠移植物进行活检,结果显示胰腺存在慢性排斥反应,十二指肠有急性炎症并伴有溃疡。就诊时,计算机断层扫描显示肠系膜积气伴肠漏,吻合口近端回肠扩张。我们进行了急诊剖腹手术,发现十二指肠非边缘性后壁有一个1.0厘米的穿孔。从穿孔部位取出未消化的富含纤维的食物,并在穿孔处覆盖一块网膜补片。在ω袢近端做了一个回肠造口术用于减压,并在附近放置了引流管。术后过程顺利。
文献中此前仅有八例移植物十二指肠穿孔的病例。富含纤维的食物残渣通过吻合口时受阻,可能导致了此次穿孔。
当患者病情稳定时,即使存在延迟性十二指肠移植物穿孔,也可能无需切除移植物。术中探查应包括对血管系统进行多普勒超声检查,以排除血栓形成作为缺血的一个因素。应进行组织活检以诊断排斥反应。