Cortez Daniel, Baturova Maria, Lindgren Arne, Carlson Jonas, Shubik Yuri V, Olsson Bertil, Platonov Pyotr G
Department of Cardiology, Clinical Sciences, Lund University, Lund, Sweden.
Electrophysiology Department, Penn State Milton S. Hershey Medical Center, Hershey, USA.
BMC Cardiovasc Disord. 2017 Jul 24;17(1):200. doi: 10.1186/s12872-017-0631-1.
Atrial fibrillation (AF) is a known risk factor for ischemic stroke. Electrocardiographic predictors of AF in population studies such as the Framingham Heart Study, as well as in hypertensive patients have demonstrated a predictive value of the P-wave duration for development of AF. QRS vector magnitude has had a predictive value in ventricular arrhythmia development. We aimed to assess the value of the three-dimensional P-wave vector magnitude and its relationship to P-wave duration for prediction of new-onset AF after ischemic stroke.
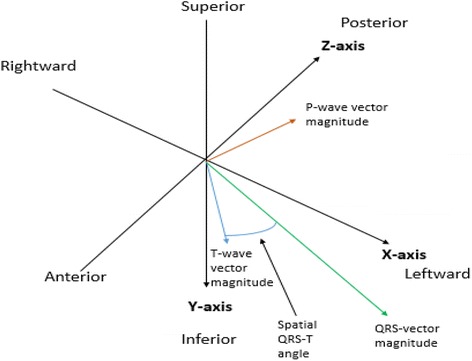
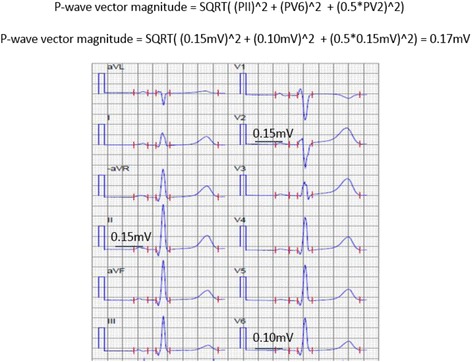
First-ever ischemic stroke patients without AF at inclusion in the Lund Stroke Register were included. Measurements of P wave duration (Pd), QRS duration, corrected QT interval, and PQ interval were performed automatically using the University of Glasgow 12-lead ECG analysis algorithm. The P-wave vector magnitude (Pvm) was calculated automatically as the square root of the sum of the squared P-wave magnitudes in leads V6, II and one half of the P-wave amplitude in V2 ([Formula: see text]), based on the P-wave magnitude (Pvm) as defined by the visually transformed Kors' Quasi-orthogonal method.
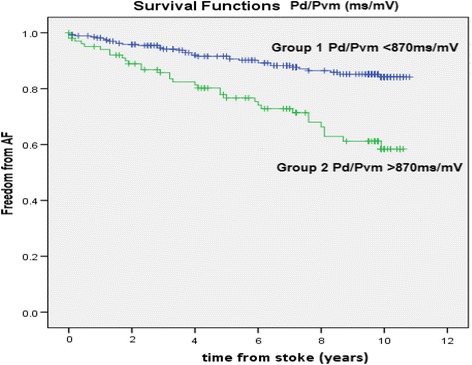
The median age was 73 (IQR 63-80) years at stroke onset (135 males, 92 females). Multivariate predictors of new-onset atrial fibrillation included age > 65 years, hypertension, and Pd/Pvm. A cut-off value of 870 ms/mV gave sensitivity, specificity, positive and negative predictive values of 51, 79, 30 and 87%, respectively. The Pd/Pvm was the only ECG predictor of AF with a significant multivariate hazard ratio of 2.02 (95% CI 1.18 to 3.46, p = 0.010).
P-wave dispersion as measured by the Pd/Pvm was the only ECG parameter measured which independently predicted subsequent AF identification in a cohort of stroke patients. Further prospective studies in larger cohorts are needed to validate its clinical usefulness.
房颤(AF)是已知的缺血性卒中危险因素。在人群研究如弗明汉心脏研究以及高血压患者中,心电图预测房颤的指标已证明P波时限对房颤发生具有预测价值。QRS向量大小对室性心律失常的发生具有预测价值。我们旨在评估三维P波向量大小及其与P波时限的关系对缺血性卒中后新发房颤的预测价值。
纳入首次发生缺血性卒中且纳入隆德卒中登记时无房颤的患者。使用格拉斯哥大学12导联心电图分析算法自动测量P波时限(Pd)、QRS时限、校正QT间期和PQ间期。基于视觉转换的科斯准正交方法定义的P波大小(Pvm),自动计算P波向量大小(Pvm),即V6、II导联P波大小平方和与V2导联P波振幅一半的平方和的平方根([公式:见原文])。
卒中发作时的中位年龄为73(四分位间距63 - 80)岁(男性135例,女性92例)。新发房颤的多变量预测因素包括年龄>65岁、高血压和Pd/Pvm。截断值为870 ms/mV时,敏感性、特异性、阳性和阴性预测值分别为51%、79%、30%和87%。Pd/Pvm是房颤唯一具有显著多变量风险比2.02(95%可信区间1.18至3.46,p = 0.010)的心电图预测指标。
通过Pd/Pvm测量的P波离散度是所测量的唯一能独立预测一组卒中患者后续房颤识别的心电图参数。需要在更大队列中进行进一步的前瞻性研究以验证其临床实用性。