Gadia Rafael, Teixeira Leite Elton Trigo, Bierrenbach Ana Luiza, Ynoe de Moraes Fabio, Spratt Daniel E, Arruda Fernando Freire, Cintra Vita Abreu Carlos Eduardo, Fernandes da Silva Joao Luis, de Andrade Carvalho Heloisa, Garicochea Bernardo
Department of Radiation Oncology, Hospital Sírio-Libanês, Brasilia, DF, Brazil.
Department of Radiation Oncology, Hospital Sírio-Libanês, São Paulo, SP, Brazil.
Adv Radiat Oncol. 2016 Oct 29;1(4):300-309. doi: 10.1016/j.adro.2016.10.006. eCollection 2016 Oct-Dec.
The addition of androgen deprivation therapy (ADT) to conventional radiation therapy improves overall survival (OS) in intermediate- and high-risk prostate cancer. The benefit of ADT to added to dose-escalated radiotherapy is less clear. The aim of this study was to report disease control outcomes and to identify prognostic variables associated with favorable outcomes in patients with intermediate- and high-risk prostate cancer treated with dose-escalated radiation therapy without ADT.
From September 2001 to March 2010, 127 patients with intermediate- or high-risk prostate cancer were treated with dose-escalated radiation otherapy without ADT. Biochemical recurrence-free survival (bRFS), distant metastases-free survival (DMFS), prostate cancer-specific mortality, and OS were assessed. Univariate and multivariate analyses using Cox regression modeling were performed.
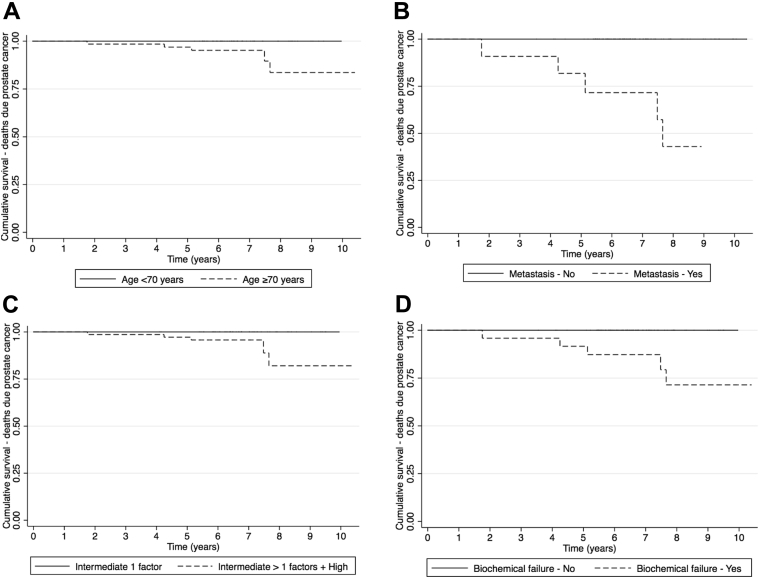
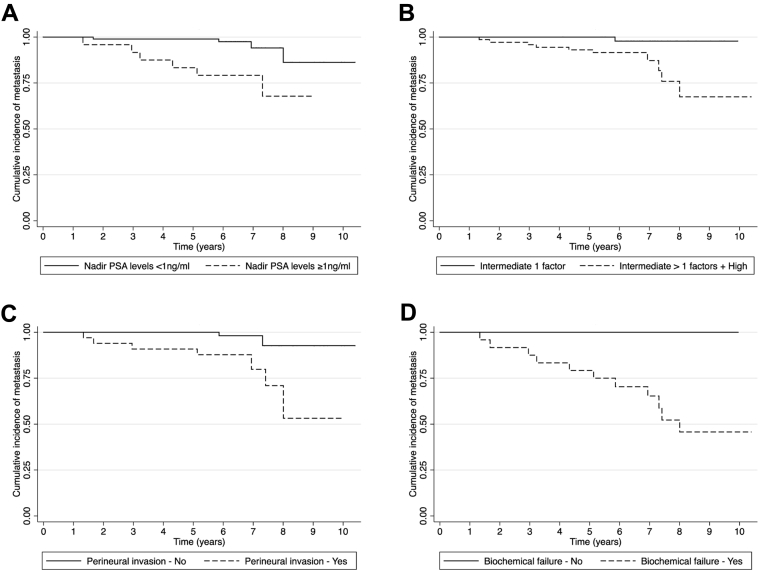
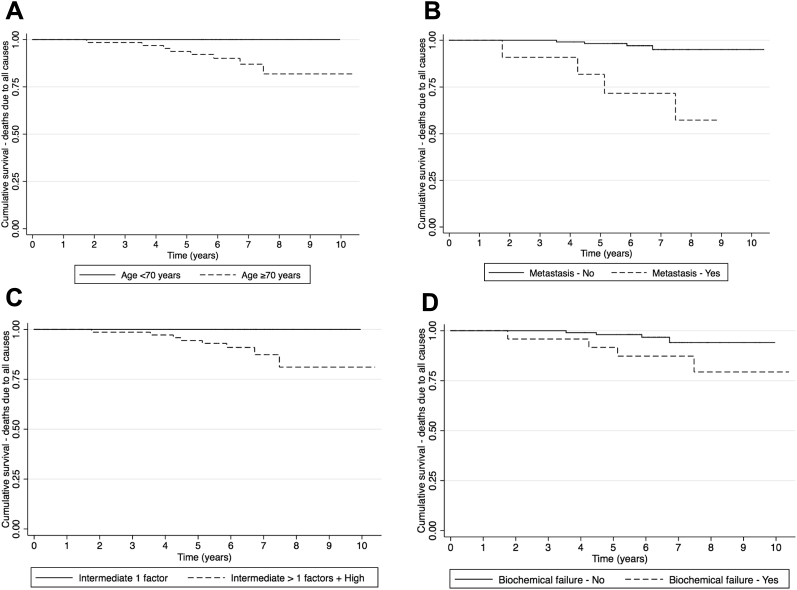
The median follow-up was 6.5 years, and the 5-year estimated bRFS, DMFS, prostate cancer-specific mortality, and OS for all patients was 89%, 96.1%, 98.4%, and 96.9% respectively. On multivariate analysis, factors that predict bRFS include risk group and PSA nadir, and factors that predict DMFS include perineural invasion, risk group, and PSA nadir.
Patients with favorable intermediate-risk cancer could likely be treated with dose-escalated radiation therapy without ADT. Patients with high-risk and unfavorable intermediate-risk cancer, perineural invasion, and PSA nadir ≥1ng/dL had worse outcomes and likely need distinct therapeutic approaches.
在传统放疗基础上加用雄激素剥夺治疗(ADT)可提高中高危前列腺癌患者的总生存期(OS)。ADT加至剂量递增放疗中的获益尚不清楚。本研究的目的是报告疾病控制结果,并确定在接受无ADT的剂量递增放疗的中高危前列腺癌患者中与良好预后相关的预后变量。
2001年9月至2010年3月,127例中高危前列腺癌患者接受了无ADT的剂量递增放疗。评估无生化复发生存期(bRFS)、无远处转移生存期(DMFS)、前列腺癌特异性死亡率和OS。使用Cox回归模型进行单因素和多因素分析。
中位随访时间为6.5年,所有患者的5年估计bRFS、DMFS、前列腺癌特异性死亡率和OS分别为89%、96.1%、98.4%和96.9%。多因素分析显示,预测bRFS的因素包括风险组和PSA最低点,预测DMFS的因素包括神经周围侵犯、风险组和PSA最低点。
预后良好的中危癌症患者可能无需ADT即可接受剂量递增放疗。高危和预后不良的中危癌症、神经周围侵犯以及PSA最低点≥1ng/dL的患者预后较差,可能需要不同的治疗方法。