Huang Ellen X, Robinson Clifford G, Molotievschi Alerson, Bradley Jeffrey D, Deasy Joseph O, Oh Jung Hun
Department of Radiation Oncology and Molecular Sciences, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Department of Radiation Oncology, Washington University School of Medicine, Saint Louis, Missouri.
Adv Radiat Oncol. 2016 Nov 16;2(1):37-43. doi: 10.1016/j.adro.2016.11.003. eCollection 2017 Jan-Mar.
Treatment planning factors are known to affect the risk of severe acute esophagitis during thoracic radiation therapy. We tested a previously published model to predict the risk of severe acute esophagitis on an independent data set.
The data set consists of data from patients who had recoverable treatment plans and received definitive radiation therapy for non-small cell carcinoma of the lung at a single institution between November 2004 and January 2010. Complete esophagus dose-volume and available clinical information was extracted using our in-house software. The previously published model was a logistic function with a combination of mean esophageal dose and use of concurrent chemotherapy. In addition to testing the previous model, we used a novel, machine learning-based method to build a maximally predictive model.
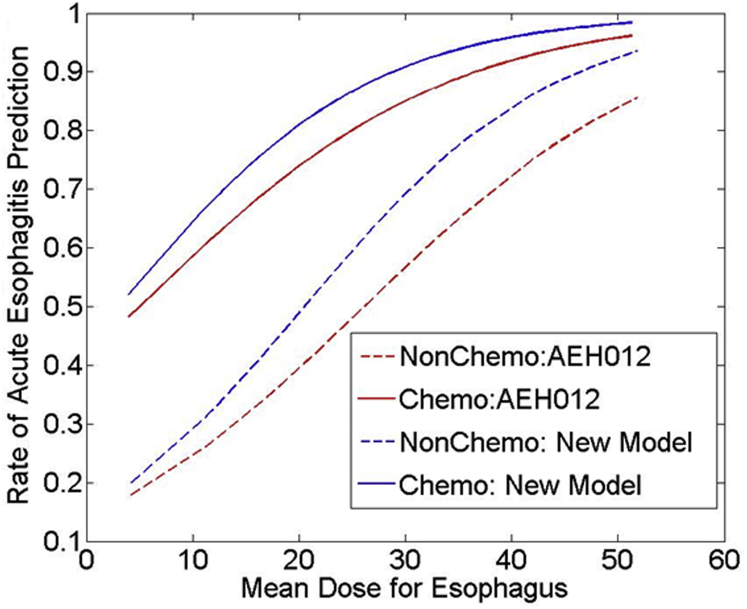
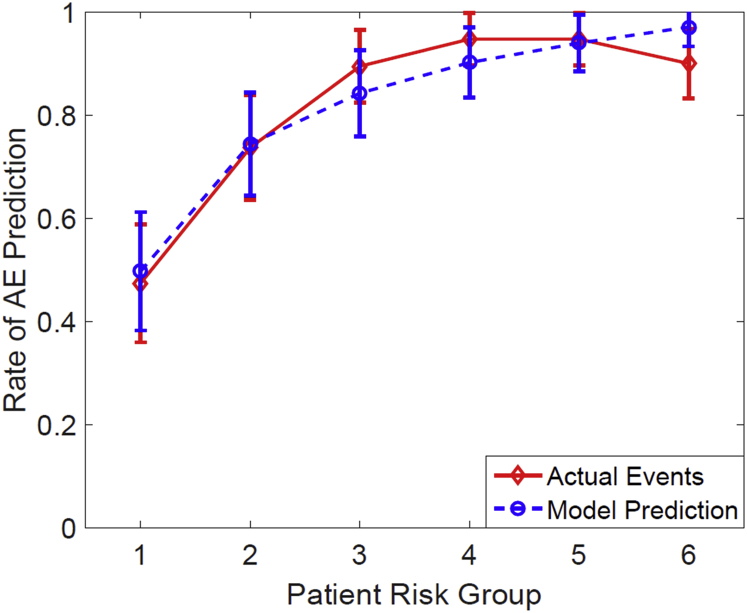
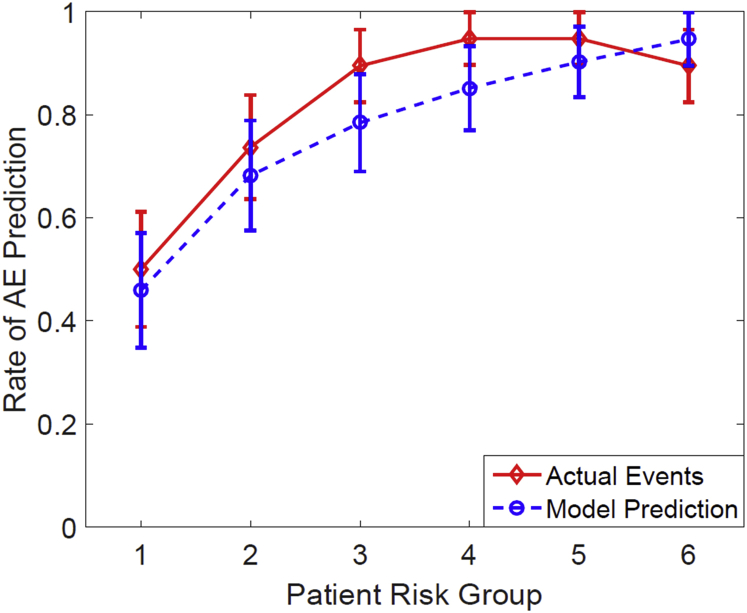
Ninety-four patients (81.7%) developed Common Terminology Criteria for Adverse Events, Version 4, Grade 2 or more severe esophagitis (Grade 2: n = 79 and Grade 3: n = 15). Univariate analysis revealed that the most statistically significant dose-volume parameters included percentage of esophagus volume receiving ≥40 to 60 Gy, minimum dose to the highest 20% of esophagus volume (D20) to D35, and mean dose. Other significant predictors included concurrent chemotherapy and patient age. The previously published model predicted risk effectively with a Spearman's rank correlation coefficient (r) of 0.43 ( < .001) with good calibration (Hosmer-Lemeshow goodness of fit: = .537). A new model that was built from the current data set found the same variables, yielding an r of 0.43 ( < .001) with a logistic function of 0.0853 × mean esophageal dose [Gy] + 1.49 × concurrent chemotherapy [1/0] - 1.75 and Hosmer-Lemeshow = .659. A novel preconditioned least absolute shrinkage and selection operator method yielded an average r of 0.38 on 100 bootstrapped data sets.
The previously published model was validated on an independent data set and determined to be nearly as predictive as the best possible two-parameter logistic model even though it overpredicted risk systematically. A novel, machine learning-based model using a bootstrapping approach showed reasonable predictive power.
已知治疗计划因素会影响胸部放射治疗期间严重急性食管炎的风险。我们在一个独立数据集上测试了一个先前发表的模型,以预测严重急性食管炎的风险。
该数据集包含2004年11月至2010年1月期间在单一机构接受可恢复治疗计划并接受非小细胞肺癌根治性放射治疗的患者的数据。使用我们的内部软件提取完整的食管剂量体积和可用的临床信息。先前发表的模型是一个逻辑函数,结合了平均食管剂量和同步化疗的使用情况。除了测试先前的模型外,我们还使用了一种基于机器学习的新方法来构建一个最大预测模型。
94名患者(81.7%)出现了不良事件通用术语标准第4版2级或更严重的食管炎(2级:n = 79;3级:n = 15)。单因素分析显示,最具统计学意义的剂量体积参数包括接受≥40至60 Gy的食管体积百分比、食管体积最高20%(D20)至D35的最小剂量以及平均剂量。其他重要的预测因素包括同步化疗和患者年龄。先前发表的模型预测风险的效果良好,Spearman等级相关系数(r)为0.43(P <.001),校准良好(Hosmer-Lemeshow拟合优度:P =.537)。从当前数据集构建的新模型发现了相同的变量,逻辑函数为0.0853×平均食管剂量[Gy]+1.49×同步化疗[1/0]-1.75,r为0.43(P <.001),Hosmer-Lemeshow P =.659。一种新颖的预处理最小绝对收缩和选择算子方法在100个自抽样数据集上的平均r为0.38。
先前发表的模型在一个独立数据集上得到了验证,尽管它系统性地高估了风险,但被确定为几乎与最佳的双参数逻辑模型具有相同的预测能力。一种基于机器学习的新颖模型,采用自抽样方法,显示出合理的预测能力。