Adams Hadie, Donnelly Joseph, Czosnyka Marek, Kolias Angelos G, Helmy Adel, Menon David K, Smielewski Peter, Hutchinson Peter J
Division of Neurosurgery, Department of Clinical Neuroscience, Addenbrooke's Hospital, University of Cambridge, Cambridge, United Kingdom.
Institute of Electronic Systems, Warsaw University of Technology, Warsaw, Poland.
PLoS Med. 2017 Jul 25;14(7):e1002353. doi: 10.1371/journal.pmed.1002353. eCollection 2017 Jul.
Both intracranial pressure (ICP) and the cerebrovascular pressure reactivity represent the dysregulation of pathways directly involved in traumatic brain injury (TBI) pathogenesis and have been used to inform clinical management. However, how these parameters evolve over time following injury and whether this evolution has any prognostic importance have not been studied.
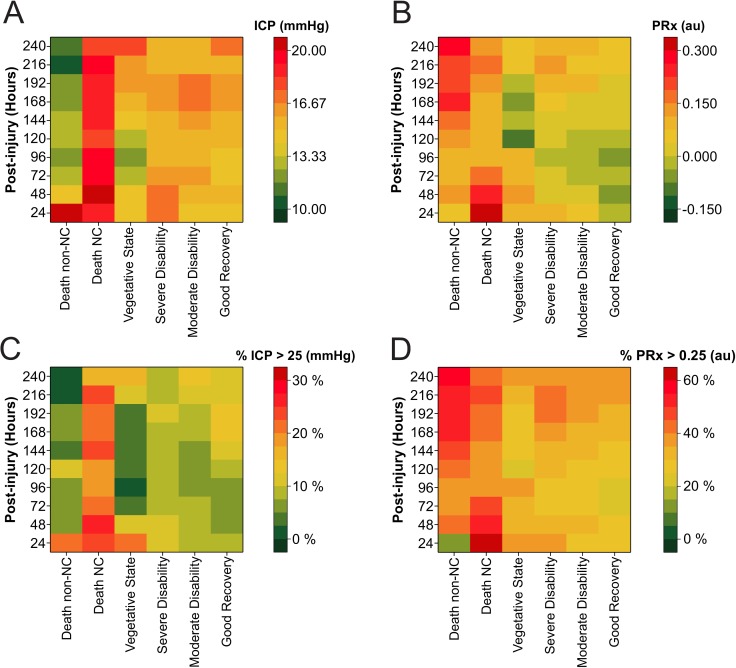
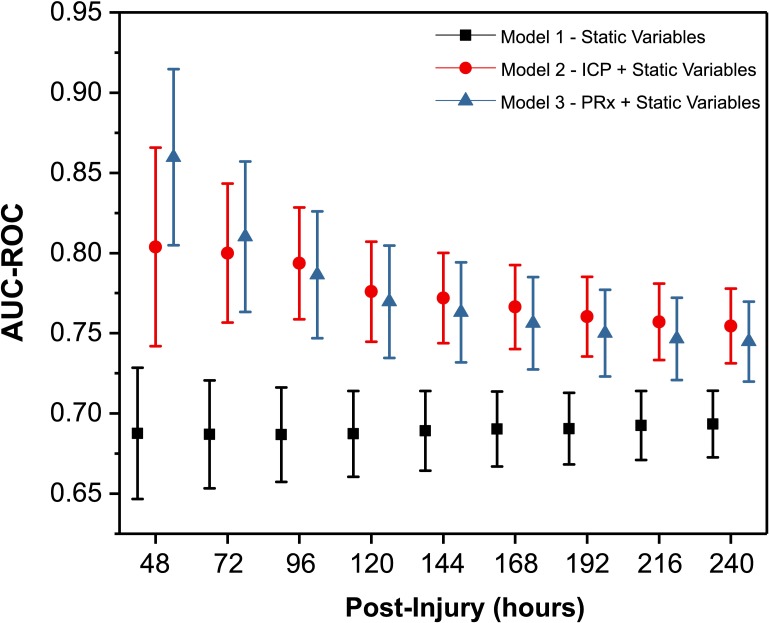
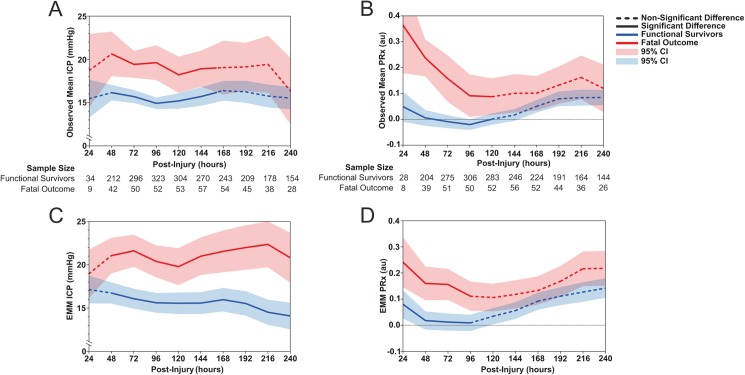
We analysed the temporal profile of ICP and pressure reactivity index (PRx), examined their relation to TBI-specific mortality, and determined if the prognostic relevance of these parameters was affected by their temporal profile using mixed models for repeated measures of ICP and PRx for the first 240 hours from the time of injury. A total of 601 adults with TBI, admitted between September 2002 to January 2016, and with high-resolution continuous monitoring from a single centre, were studied. At 6 months postinjury, 133 (19%) patients had a fatal outcome; of those, 88 (78%) died from nonsurvivable TBI or brain death. The difference in mean ICP between those with a fatal outcome and functional survivors was only significant for the first 168 hours after injury (all p < 0.05). For PRx, those patients with a fatal outcome also had a higher (more impaired) PRx throughout the first 120 hours after injury (all p < 0.05). The separation of ICP and PRx was greatest in the first 72 hours after injury. Mixed models demonstrated that the explanatory power of the PRx decreases over time; therefore, the prognostic weight assigned to PRx should similarly decrease. However, the ability of ICP to predict a fatal outcome remained relatively stable over time. As control of ICP is the central purpose of TBI management, it is likely that some of the information that is reflected in the natural history of ICP changes is no longer apparent because of therapeutic intervention.
We demonstrated the temporal evolution of ICP and PRx and their relationship with fatal outcome, indicating a potential early prognostic and therapeutic window. The combination of dynamic monitoring variables and their time profile improved prediction of outcome. Therefore, time-driven dynamic modelling of outcome in patients with severe TBI may allow for more accurate and clinically useful prediction models. Further research is needed to confirm and expand on these findings.
颅内压(ICP)和脑血管压力反应性均代表了直接参与创伤性脑损伤(TBI)发病机制的通路失调,并已用于指导临床管理。然而,这些参数在受伤后如何随时间演变以及这种演变是否具有任何预后意义尚未得到研究。
我们分析了ICP和压力反应性指数(PRx)的时间变化情况,研究了它们与TBI特异性死亡率的关系,并使用受伤后最初240小时内ICP和PRx的重复测量混合模型,确定这些参数的预后相关性是否受其时间变化情况的影响。共研究了601例2002年9月至2016年1月间收治的、来自单一中心进行高分辨率连续监测的TBI成年患者。受伤后6个月时,133例(19%)患者出现致命结局;其中,88例(78%)死于不可存活的TBI或脑死亡。致命结局患者与功能存活者之间的平均ICP差异仅在受伤后的前168小时有统计学意义(所有p<0.05)。对于PRx,致命结局患者在受伤后的前120小时内PRx也更高(受损更严重)(所有p<0.05)。ICP和PRx在受伤后的前72小时内分离最大。混合模型表明,PRx的解释力随时间下降;因此,赋予PRx的预后权重也应相应降低。然而,ICP预测致命结局的能力随时间保持相对稳定。由于控制ICP是TBI管理的核心目标,由于治疗干预,ICP变化自然史中反映的一些信息可能不再明显。
我们展示了ICP和PRx的时间演变及其与致命结局的关系,表明存在潜在的早期预后和治疗窗口。动态监测变量及其时间变化情况的结合改善了结预测。因此,对重度TBI患者的结局进行时间驱动的动态建模可能会产生更准确且临床有用的预测模型。需要进一步的研究来证实和扩展这些发现。