Pulignano Giovanni, Gulizia Michele Massimo, Baldasseroni Samuele, Bedogni Francesco, Cioffi Giovanni, Indolfi Ciro, Romeo Francesco, Murrone Adriano, Musumeci Francesco, Parolari Alessandro, Patanè Leonardo, Pino Paolo Giuseppe, Mongiardo Annalisa, Spaccarotella Carmen, Di Bartolomeo Roberto, Musumeci Giuseppe
Cardiology Department 1, Ospedale San Camillo-Forlanini, Via O. Regnoli, 8 00152 Rome, Italy.
Cardiology Department, Ospedale Garibaldi-Nesima, Azienda di Rilievo Nazionale e Alta Specializzazione "Garibaldi" Catania, Italy.
Eur Heart J Suppl. 2017 May;19(Suppl D):D354-D369. doi: 10.1093/eurheartj/sux012. Epub 2017 May 2.
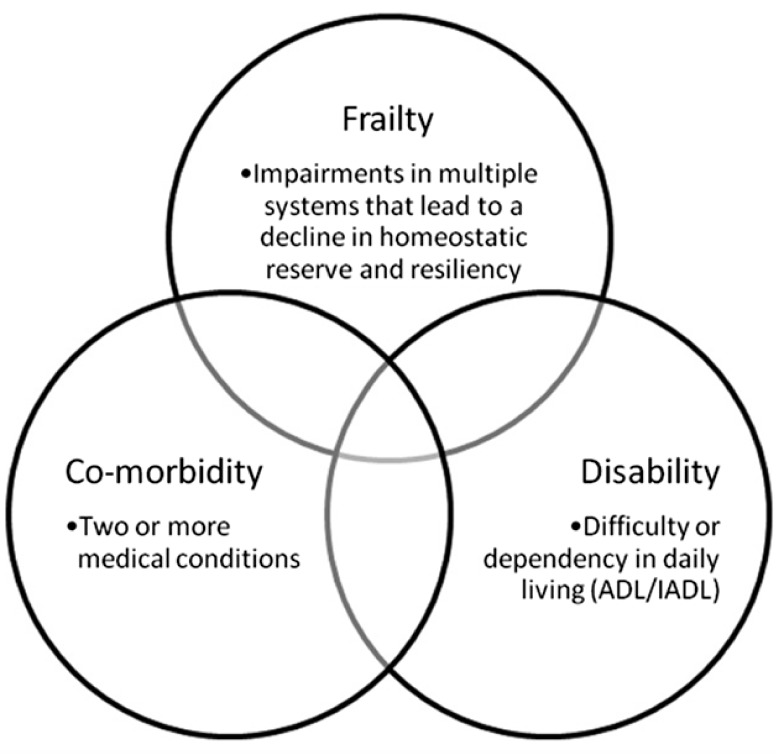
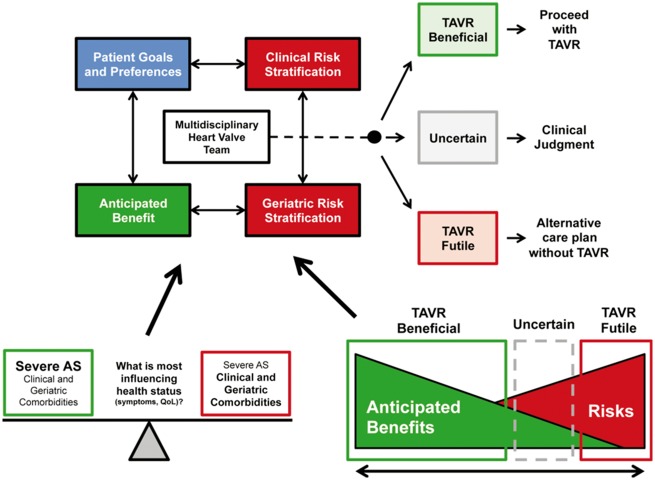
Aortic stenosis is one of the most frequent valvular diseases in developed countries, and its impact on public health resources and assistance is increasing. A substantial proportion of elderly people with severe aortic stenosis is not eligible to surgery because of the advanced age, frailty, and multiple co-morbidities. Transcatheter aortic valve implantation (TAVI) enables the treatment of very elderly patients at high or prohibitive surgical risk considered ineligible for surgery and with an acceptable life expectancy. However, a significant percentage of patients die or show no improvement in quality of life (QOL) in the follow-up. In the decision-making process, it is important to determine: (i) whether and how much frailty of the patient influences the risk of procedures; (ii) how the QOL and the individual patient's survival are influenced by aortic valve disease or from other associated conditions; and (iii) whether a geriatric specialist intervention to evaluate and correct frailty or other diseases with their potential or already manifest disabilities can improve the outcome of surgery or TAVI. Consequently, in addition to risk stratification with conventional tools, a number of factors including multi-morbidity, disability, frailty, and cognitive function should be considered, in order to assess the expected benefit of both surgery and TAVI. The pre-operative optimization through a multidisciplinary approach with a Heart Team can counteract the multiple damage (cardiac, neurological, muscular, respiratory, and kidney) that can potentially aggravate the reduced physiological reserves characteristic of frailty. The systematic application in clinical practice of multidimensional assessment instruments of frailty and cognitive function in the screening and the adoption of specific care pathways should facilitate this task.
在发达国家,主动脉瓣狭窄是最常见的瓣膜疾病之一,其对公共卫生资源和医疗救助的影响日益增大。相当一部分患有严重主动脉瓣狭窄的老年人由于年龄较大、身体虚弱以及多种合并症而不适合接受手术。经导管主动脉瓣植入术(TAVI)能够治疗那些因手术风险高或被认为手术禁忌而不适合手术但预期寿命尚可的高龄患者。然而,在随访中有相当比例的患者死亡或生活质量(QOL)并无改善。在决策过程中,确定以下几点很重要:(i)患者的虚弱程度是否以及在多大程度上会影响手术风险;(ii)主动脉瓣疾病或其他相关疾病如何影响患者的生活质量和个体生存;(iii)老年专科医生进行干预以评估和纠正虚弱或其他伴有潜在或已显现残疾的疾病,是否能够改善手术或TAVI的结果。因此,除了使用传统工具进行风险分层外,还应考虑包括多种合并症、残疾、虚弱和认知功能等在内的诸多因素,以便评估手术和TAVI的预期获益。通过心脏团队采用多学科方法进行术前优化,可以抵消可能加重虚弱所特有的生理储备降低的多种损害(心脏、神经、肌肉、呼吸和肾脏方面的损害)。在临床实践中系统应用虚弱和认知功能的多维评估工具进行筛查,并采用特定的护理路径,应有助于完成这项任务。