Asgeirsson Daniel, Hedström Erik, Jögi Jonas, Pahlm Ulrika, Steding-Ehrenborg Katarina, Engblom Henrik, Arheden Håkan, Carlsson Marcus
Department of Clinical Sciences Lund, Clinical Physiology, Lund University, Skane University Hospital, Lund, Sweden.
Department of Clinical Sciences Lund, Diagnostic Radiology, Lund University, Skane University Hospital, Lund, Sweden.
BMC Cardiovasc Disord. 2017 Jul 28;17(1):208. doi: 10.1186/s12872-017-0641-z.
The majority (60%) of left ventricular (LV) stroke volume (SV) is generated by longitudinal shortening causing apical atrioventricular plane displacement (AVPD) in systole. The remaining SV is caused by radial inward motion of the epicardium both in the septal and the lateral wall. We aimed to determine if these longitudinal, septal and lateral contributions to LVSV are changed in patients with chronic myocardial infarction (MI).
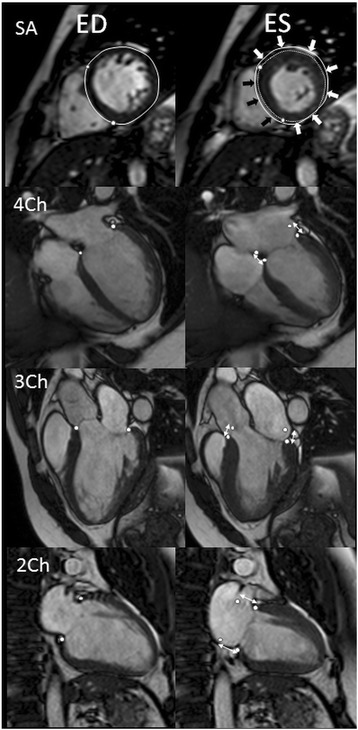
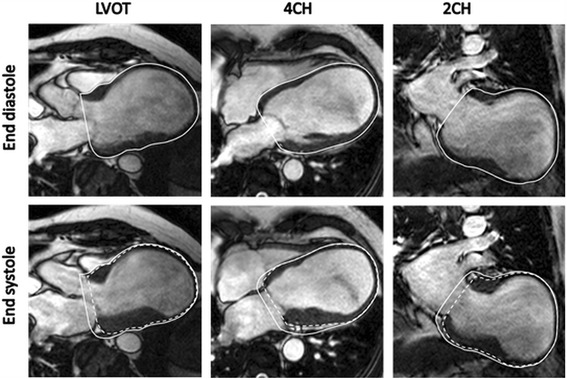
Patients with a chronic (>3 months) ST-elevation MI in the left anterior descending (LAD, n = 20) or right coronary artery (RCA, n = 16) and healthy controls (n = 20) were examined with cardiovascular magnetic resonance (CMR). AVPD was quantified in long axis cine CMR images and LV volumes and dimensions in short axis cine images.
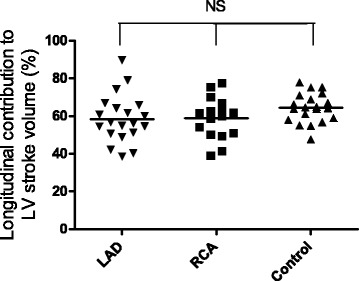
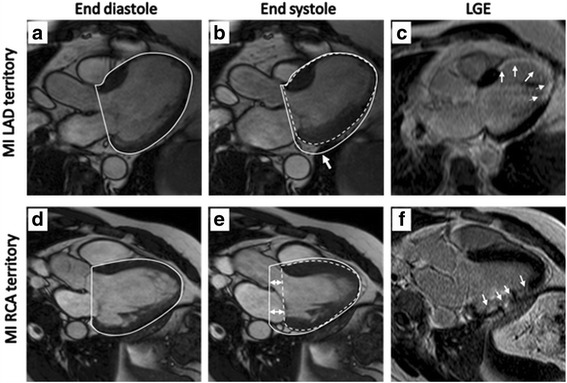
AVPD was decreased both in patients with LAD-MI (11 ± 1 mm, p < 0.001) and RCA-MI (13 ± 1 mm, p < 0.05) compared to controls (15 ± 0 mm). However, the longitudinal contribution to SV was unchanged for both LAD-MI (58 ± 3%, p = 0.08) and RCA-MI (59 ± 3%, p = 0.09) compared to controls (64 ± 2%). The preserved longitudinal contribution despite decreased absolute AVPD was a results of increased epicardial dimensions (p < 0.01 for LAD-MI and p = 0.06 for RCA-MI). In LAD-MI the septal contribution to LVSV was decreased (5 ± 1%) compared to both controls (10 ± 1%, p < 0.01) and patients with RCA-MIs (10 ± 1%, p < 0.01). The lateral contribution was increased in LAD-MI patients (44 ± 3%) compared to both RCA-MI (35 ± 2%, p < 0.05) and controls (29 ± 2%, p < 0.001).
Longitudinal shortening remains the principal component of left ventricular pumping in patients with chronic MI even when the absolute AVPD is decreased.
左心室(LV)每搏输出量(SV)的大部分(60%)是由纵向缩短产生的,在收缩期导致心尖房室平面位移(AVPD)。其余的SV是由室间隔和侧壁的心外膜径向向内运动引起的。我们旨在确定慢性心肌梗死(MI)患者中这些对左心室每搏输出量的纵向、室间隔和侧壁的贡献是否发生改变。
对左前降支(LAD,n = 20)或右冠状动脉(RCA,n = 16)发生慢性(>3个月)ST段抬高型心肌梗死的患者以及健康对照者(n = 20)进行心血管磁共振(CMR)检查。在长轴电影CMR图像中对AVPD进行定量,在短轴电影图像中对左心室容积和尺寸进行测量。
与对照组(15±0 mm)相比,LAD-MI患者(11±1 mm,p < 0.001)和RCA-MI患者(13±1 mm,p < 0.05)的AVPD均降低。然而,与对照组(64±2%)相比,LAD-MI(58±3%,p = 0.08)和RCA-MI(59±3%,p = 0.09)对每搏输出量的纵向贡献没有变化。尽管绝对AVPD降低,但纵向贡献得以保留是心外膜尺寸增加的结果(LAD-MI为p < 0.01,RCA-MI为p = 0.06)。与对照组(10±1%,p < 0.01)和RCA-MI患者(10±1%,p < 0.01)相比,LAD-MI患者对左心室每搏输出量的室间隔贡献降低(5±1%)。与RCA-MI患者(35±2%,p < 0.05)和对照组(29±2%,p < 0.001)相比,LAD-MI患者的侧壁贡献增加(44±3%)。
即使绝对AVPD降低,纵向缩短仍是慢性心肌梗死患者左心室泵血的主要组成部分。