Freedman Barry I, Rocco Michael V, Bates Jeffrey T, Chonchol Michel, Hawfield Amret T, Lash James P, Papademetriou Vasilios, Sedor John R, Servilla Karen, Kimmel Paul L, Wall Barry M, Pajewski Nicholas M
Department of Internal Medicine, Section on Nephrology; Wake Forest School of Medicine, Winston-Salem, NC.
Michael E. DeBakey Veterans Administration Medical Center and Baylor College of Medicine, Houston, TX.
Kidney Int Rep. 2017 Jul;2(4):713-720. doi: 10.1016/j.ekir.2017.03.008. Epub 2017 Mar 31.
Relationships between apolipoprotein L1 gene () renal-risk variants (RRVs) and cardiovascular disease (CVD) remain controversial. To clarify associations between and CVD, 2,568 African American Systolic Blood Pressure Intervention Trial (SPRINT) participants were assessed for the incidence of CVD events (primary composite including non-fatal myocardial infarction, acute coronary syndrome not resulting in myocardial infarction, nonfatal stroke, non-fatal acute decompensated heart failure, and CVD death), renal outcomes, and all-cause mortality.
Cox proportional hazards regression models were employed adjusting for age, sex, African ancestry proportion, and treatment group (systolic blood pressure target of <120 mm Hg versus <140 mm Hg).
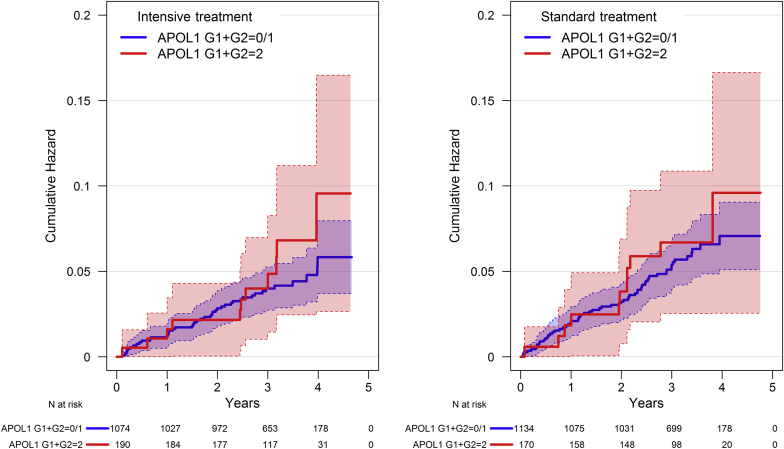
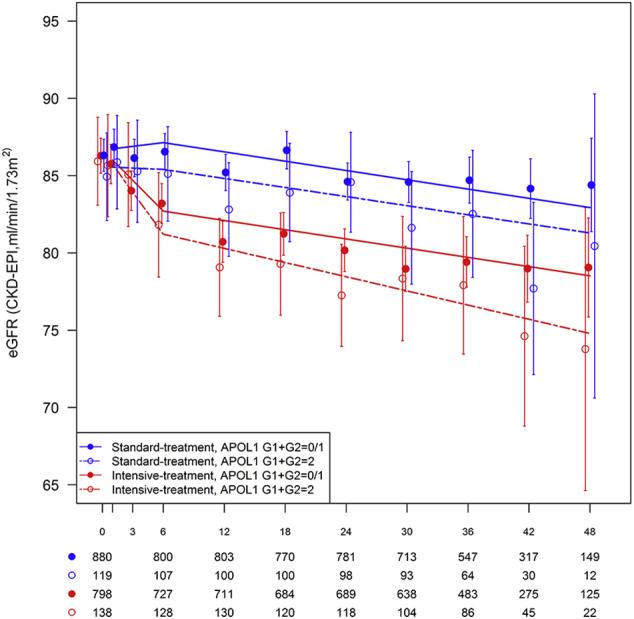
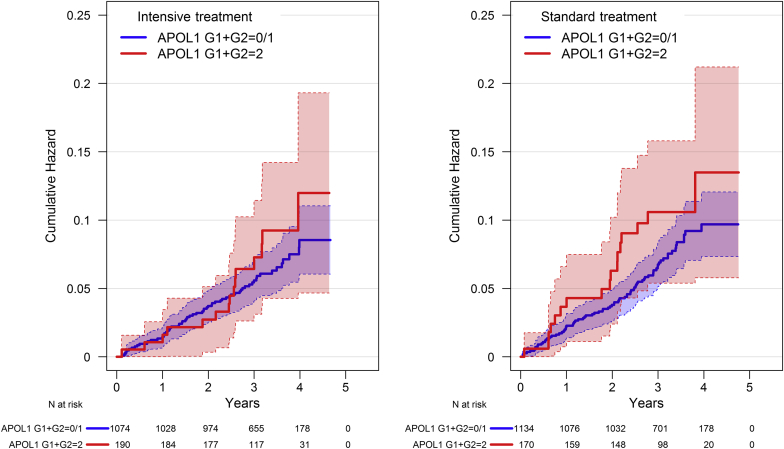
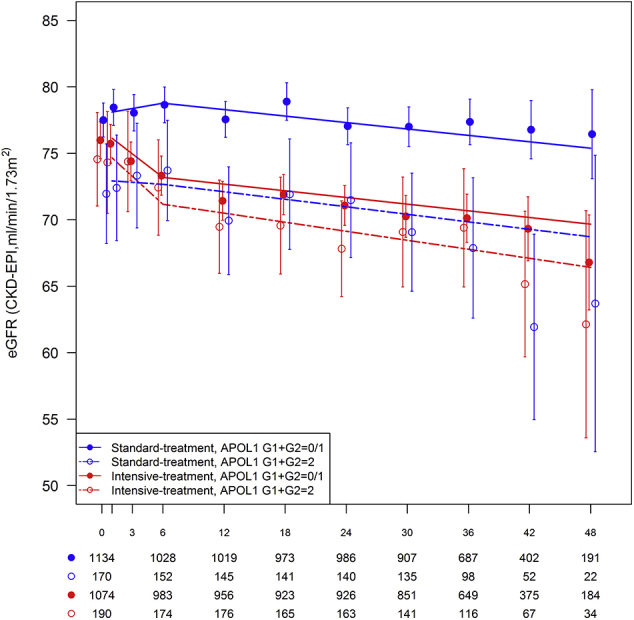
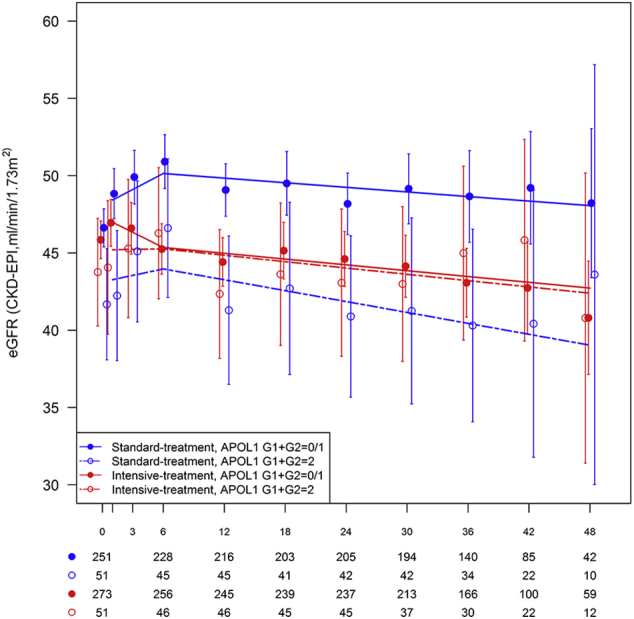
Fourteen percent of participants had two RRVs; these individuals also had lower baseline estimated GFR and higher levels of albuminuria and BMI. After a median follow-up of 39 months, no significant association was observed between RRVs and the primary composite CVD outcome, any of its components, or all-cause mortality (recessive or additive genetic models). demonstrated a trend toward association with sustained 30% reduction in estimated GFR to <60 ml/min/1.73m in those with normal kidney function at baseline (hazard ratio [95% CI] 1.64 [0.85-2.93]; p=0.114, recessive model).
RRVs were not associated with incident CVD in high-risk hypertensive, non-diabetic African American participants in SPRINT.
载脂蛋白L1基因()的肾脏风险变异(RRV)与心血管疾病(CVD)之间的关系仍存在争议。为了阐明与CVD之间的关联,对2568名非裔美国收缩压干预试验(SPRINT)参与者的CVD事件发生率(主要复合终点包括非致死性心肌梗死、未导致心肌梗死的急性冠状动脉综合征、非致死性中风、非致死性急性失代偿性心力衰竭和CVD死亡)、肾脏结局和全因死亡率进行了评估。
采用Cox比例风险回归模型,并对年龄、性别、非洲血统比例和治疗组(收缩压目标为<120mmHg与<140mmHg)进行了调整。
14%的参与者有两个RRV;这些个体的基线估计肾小球滤过率也较低,蛋白尿水平和体重指数较高。在中位随访39个月后,未观察到RRV与主要复合CVD结局、其任何组成部分或全因死亡率之间存在显著关联(隐性或加性遗传模型)。在基线时肾功能正常的参与者中,显示出与估计肾小球滤过率持续降低30%至<60ml/min/1.73m²相关的趋势(风险比[95%置信区间]1.64[0.85-2.93];p=0.114,隐性模型)。
在SPRINT中,高风险高血压、非糖尿病非裔美国参与者的RRV与新发CVD无关。