Weng Wayne, Tian Ye, Kimball Edward S, Kong Sheldon X, Bouchard Jonathan, Hobbs Todd M, Sakurada Brian
Department of Health and Economics Outcomes Research, Novo Nordisk, Plainsboro, New Jersey, USA.
Medical Writing and Education, Novo Nordisk, Plainsboro, New Jersey, USA.
BMJ Open Diabetes Res Care. 2017 May 27;5(1):e000382. doi: 10.1136/bmjdrc-2016-000382. eCollection 2017.
This study evaluated relationships between glycaemic control, body mass index (BMI), comorbidities and pharmacological treatment in patients with type 2 diabetes mellitus (T2D).
This was a retrospective, cross-sectional analysis of Quintiles electronic medical records research data (study period 1 October 2013-30 September 2014). Eligibility included age ≥18 years, T2D diagnosis, and at least one available BMI measurement.
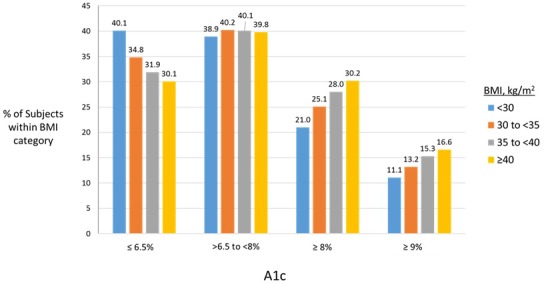
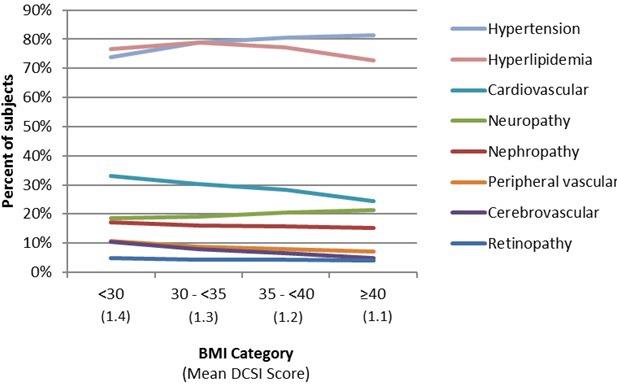
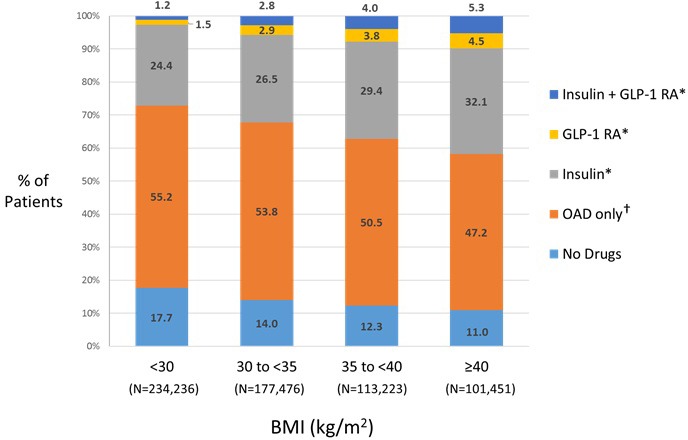
The study included 626 386 patients (mean age, 63.8 year; 51.3% female; 78.5% white; 62.6%, BMI ≥30 kg/m). A1c data were available for 414 266 patients. The proportion of patients with good glycaemic control (A1c ≤6.5) decreased as BMI category increased, ranging from 40.1% of patients with BMI <30% to 30.1% of patients with BMI ≥40. The proportions of patients with poor glycaemic control (A1c >8% and A1c ≥9%) increased with increasing BMI category. Oral antidiabetic drugs (OAD) were the most frequently used (54.4% of patients with A1c values). Among patients using insulin-based therapy, 50% had an A1c ≥8% and 29% had an A1c ≥9% regardless of concomitant OAD or glucagon-like peptide 1 receptor agonist use. Among patients using three or more OADs, 34.3% and 16.1% had A1c values ≥8% and ≥9%, respectively. There was no common trend observed for changes in the proportion of patients with T2D-related comorbidities according to BMI category. The most notable trend was a 7.6% net increase in the percentage of patients with hypertension from BMI <30 to BMI ≥40.
This large dataset provides evidence that roughly one out of four patients with T2D is not well controlled, and the prevalence of poor glycaemic control increases as BMI increases.
本研究评估了2型糖尿病(T2D)患者的血糖控制、体重指数(BMI)、合并症与药物治疗之间的关系。
这是一项对昆泰电子病历研究数据进行的回顾性横断面分析(研究期为2013年10月1日至2014年9月30日)。纳入标准包括年龄≥18岁、T2D诊断以及至少一次可用的BMI测量值。
该研究纳入了626386名患者(平均年龄63.8岁;51.3%为女性;78.5%为白人;62.6%的BMI≥30kg/m²)。414266名患者有糖化血红蛋白(A1c)数据。随着BMI类别增加,血糖控制良好(A1c≤6.5)的患者比例下降,范围从BMI<30kg/m²的患者中的40.1%到BMI≥40kg/m²的患者中的30.1%。血糖控制不佳(A1c>8%和A1c≥9%)的患者比例随着BMI类别增加而上升。口服降糖药(OAD)是最常用的药物(糖化血红蛋白值患者中的54.4%)。在使用胰岛素治疗的患者中,无论是否同时使用OAD或胰高血糖素样肽1受体激动剂,50%的患者A1c≥8%,29%的患者A1c≥9%。在使用三种或更多种OAD的患者中,分别有34.3%和16.1%的患者糖化血红蛋白值≥8%和≥9%。未观察到根据BMI类别T2D相关合并症患者比例变化的共同趋势。最显著的趋势是高血压患者百分比从BMI<30kg/m²到BMI≥40kg/m²净增加7.6%。
这个大型数据集提供了证据,表明大约四分之一的T2D患者血糖控制不佳,且血糖控制不佳的患病率随着BMI增加而上升。