Health Economics Research Centre, Nuffield Department of Population Health, University of Oxford, Old Road Campus, Headington, Oxford, OX3 7LF, UK.
Oxford Molecular Diagnostics Centre, Oxford University Hospitals Trust, Oxford, UK.
Pharmacoeconomics. 2017 Aug;35(8):845-858. doi: 10.1007/s40273-017-0519-z.
Genomic tests may improve the stratification of patients to receive new therapies in several disease areas. However, the use of expensive targeted therapies can impact on the cost effectiveness of these tests. This study presents an economic evaluation of genomic testing in chronic lymphocytic leukaemia in the context of the UK National Health Service.
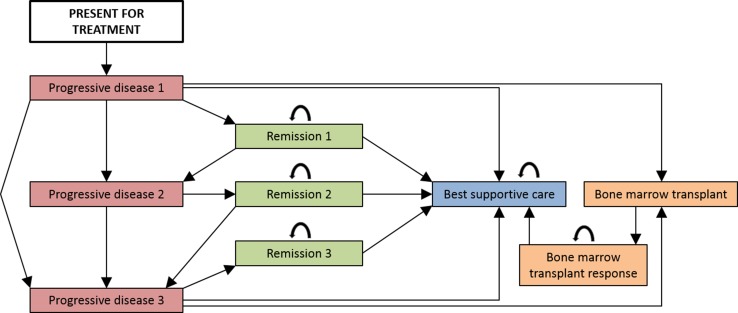
Cost-effectiveness and cost-utility analyses (using life-years and quality-adjusted life-years) were undertaken from a National Health Service and societal perspective. Five strategies were evaluated across several age groups using Markov modelling: three strategies that reflected varying current genetic testing practice and two configurations of genomic testing (including ibrutinib treatment).
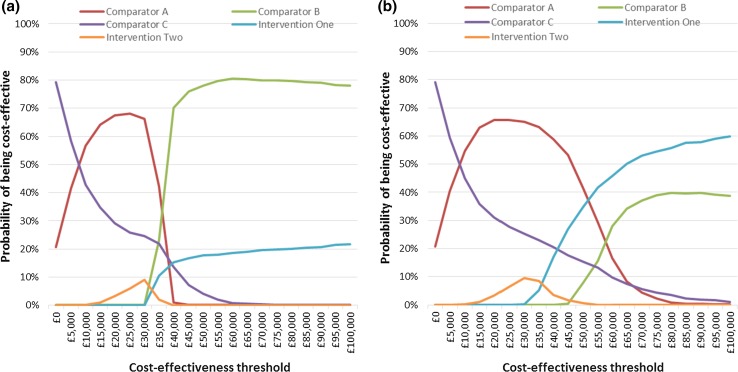
Genomic testing strategies yielded the most life-years/quality-adjusted life-years per patient, but were not cost effective compared with a threshold of £30,000 per life-year/quality-adjusted life-year gained. Cost-effectiveness acceptability curves indicated that there was some uncertainty surrounding this result. A genomic testing strategy becomes the most cost-effective option if a higher end-of-life cost-effectiveness threshold of £50,000 is applied, if a societal costing perspective is considered in 25-year-old patients or if the cost of ibrutinib treatment falls.
Stratifying patients with chronic lymphocytic leukaemia to targeted treatment using genomic testing improves health outcomes, but will likely only represent a cost-effective use of limited National Health Service resources if a higher cost-effectiveness threshold or societal costing perspective is applied, or if the price of ibrutinib treatment is reduced. This result may be broadly indicative of the likely cost effectiveness of other genomic tests that inform the stratification of patients to high cost-targeted therapies.
基因组测试可以改善多个疾病领域的患者分层,以接受新疗法。然而,昂贵的靶向治疗的使用会影响这些测试的成本效益。本研究在英国国家医疗服务体系的背景下,对慢性淋巴细胞白血病的基因组测试进行了经济评估。
从国家医疗服务体系和社会角度进行成本效益和成本效用分析(使用生命年和质量调整生命年)。使用马尔可夫模型对几个年龄组的五种策略进行了评估:反映当前不同基因测试实践的三种策略和两种基因组测试配置(包括伊布替尼治疗)。
基因组测试策略为每位患者带来了最多的生命年/质量调整生命年,但与获得每生命年/质量调整生命年 30,000 英镑的阈值相比,并不具有成本效益。成本效益接受性曲线表明,这一结果存在一定的不确定性。如果应用更高的终末成本效益阈值 50,000 英镑,如果考虑 25 岁患者的社会成本视角,或者伊布替尼治疗的成本下降,基因组测试策略将成为最具成本效益的选择。
使用基因组测试对慢性淋巴细胞白血病患者进行靶向治疗分层可改善健康结果,但如果应用更高的成本效益阈值或社会成本视角,或者伊布替尼治疗的价格降低,那么这种测试可能仅代表对有限的国家医疗服务资源的具有成本效益的利用。这一结果可能广泛表明其他基因组测试用于指导患者分层接受高成本靶向治疗的成本效益。