Jiménez Fonseca Paula, Carmona-Bayonas Alberto, Hernández Raquel, Custodio Ana, Cano Juana Maria, Lacalle Alejandra, Echavarria Isabel, Macias Ismael, Mangas Monserrat, Visa Laura, Buxo Elvira, Álvarez Manceñido Felipe, Viudez Antonio, Pericay Carles, Azkarate Aitor, Ramchandani Avinash, López Carlos, Martinez de Castro Eva, Fernández Montes Ana, Longo Federico, Sánchez Bayona Rodrigo, Limón Maria Luisa, Diaz-Serrano Asun, Martin Carnicero Alfonso, Arias David, Cerdà Paula, Rivera Fernando, Vieitez Jose Maria, Sánchez Cánovas Manuel, Garrido M, Gallego J
Department of Medical Oncology, Central de Asturias University Hospital, Oviedo 33011, Spain.
Department of Hematology and Medical Oncology, Morales Meseguer University Hospital, Murcia 30008, Spain.
Br J Cancer. 2017 Sep 5;117(6):775-782. doi: 10.1038/bjc.2017.245. Epub 2017 Aug 1.
The choice of chemotherapy in HER2-negative gastric cancer is based on centre's preferences and adverse effects profile. No schedule is currently accepted as standard, nor are there any factors to predict response, other than HER2 status. We seek to evaluate whether Lauren type influences the efficacy of various chemotherapies and on patient overall survival (OS).
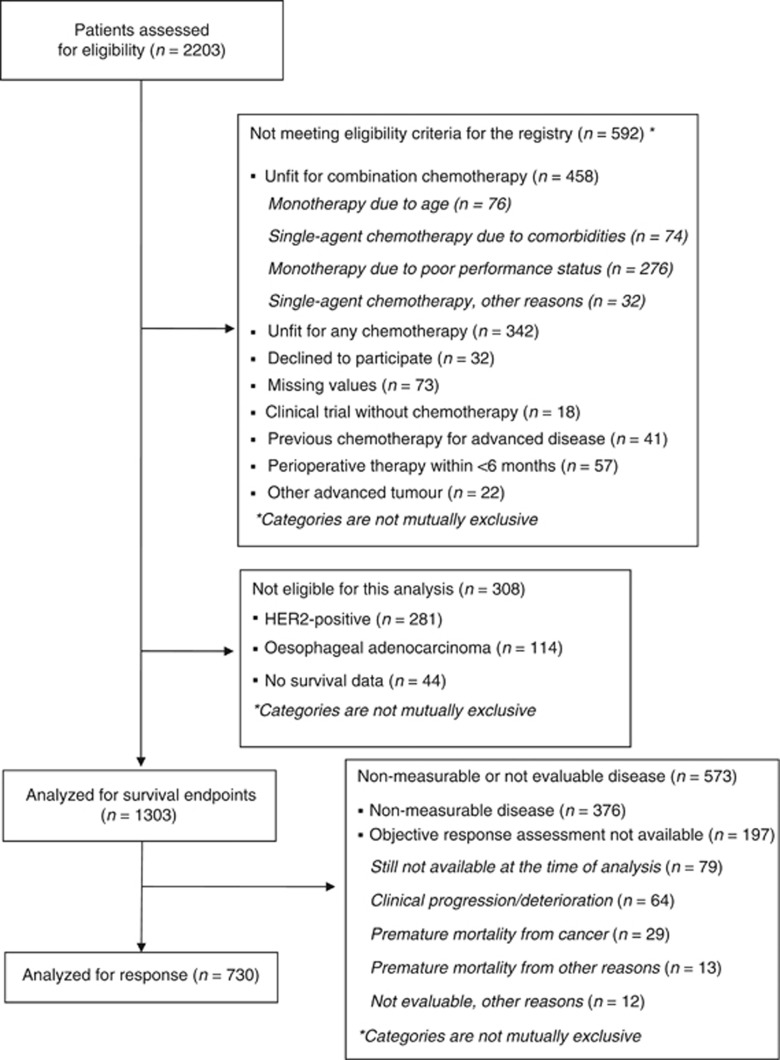
We have conducted a multicenter study in 31 hospitals. The eligibility criteria include diagnosis of stomach or gastroesophageal junction adenocarcinoma, HER2 negativity, and chemotherapy containing 2-3 drugs. Cox proportional hazards regression adjusted for confounding factors, with tests of 'treatment-by-histology' interaction, was used to estimate treatment effect.
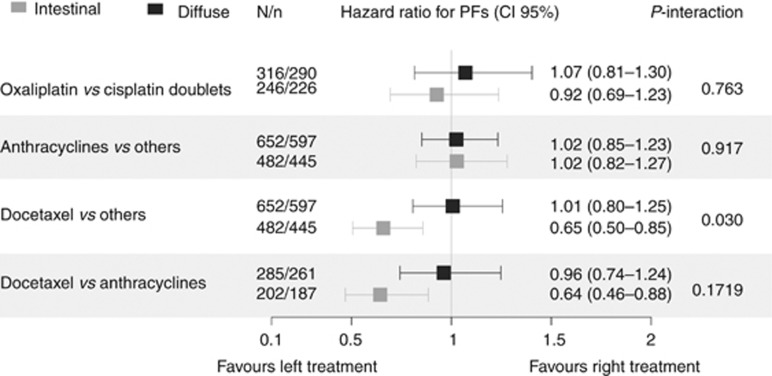
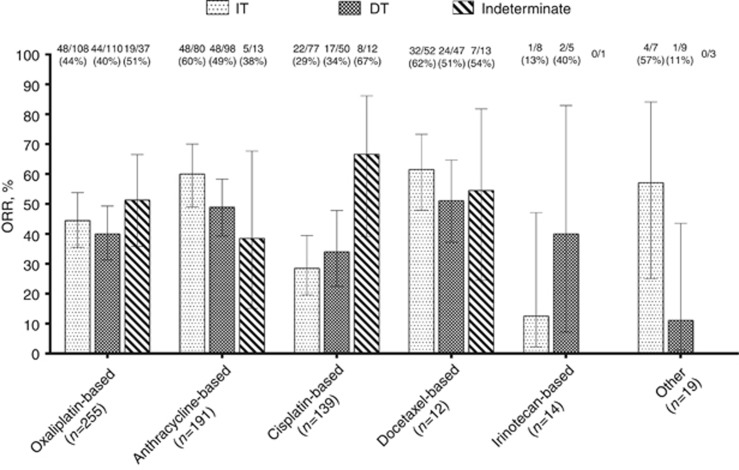
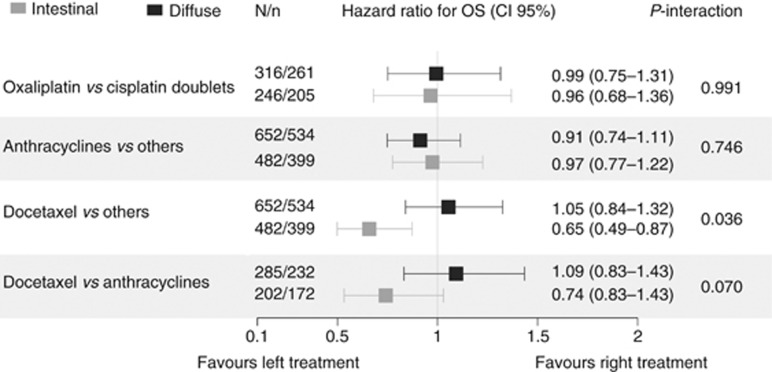
Our registry contains 1303 tumours analysable for OS end points and 730 evaluable for overall response rate (ORR). A decrease in ORR was detected in the presence of a diffuse component: odds ratio 0.719 (95% confidence interval (CI), 0.525-0.987), P=0.039. Anthracycline- or docetaxel-containing schedules increased ORR only in the intestinal type. The diffuse type displayed increased mortality with hazard ratio (HR) of 1.201 (95% CI, 1.054-1.368), P=0.0056. Patients receiving chemotherapy with docetaxel exhibited increased OS limited to the intestinal type: HR 0.65 (95% CI, 0.49-0.87), P=0.024, with no increment in OS for the subset having a diffuse component. With respect to progression-free survival (PFS), a significant interaction was seen in the effect of docetaxel-containing schedules, with better PFS limited to the intestinal type subgroup, in the comparison against any other schedule: HR 0.65 (95% CI, 0.50-0.85), P=0.015, and against anthracycline-based regimens: HR 0.64 (95% CI, 0.46-0.88), P=0.046.
As a conclusion, in this registry, Lauren classification tumour subtypes predicted survival and responded differently to chemotherapy. Future clinical trials should stratify effect estimations based on histology.
人表皮生长因子受体2(HER2)阴性胃癌的化疗方案选择基于各中心的偏好及不良反应情况。目前尚无标准化的化疗方案,除HER2状态外,也没有其他预测疗效的因素。我们旨在评估劳伦分型是否会影响各种化疗方案的疗效及患者总生存期(OS)。
我们在31家医院开展了一项多中心研究。纳入标准包括胃或胃食管交界腺癌的诊断、HER2阴性以及含2 - 3种药物的化疗。采用经混杂因素校正的Cox比例风险回归模型,并进行“治疗与组织学”交互作用检验,以评估治疗效果。
我们的登记数据库包含1303例可用于OS终点分析的肿瘤病例以及730例可评估总缓解率(ORR)的病例。发现存在弥漫性成分时ORR降低:比值比为0.719(95%置信区间(CI),0.525 - 0.987),P = 0.039。含蒽环类药物或多西他赛的化疗方案仅在肠型中提高了ORR。弥漫型显示死亡率增加,风险比(HR)为1.201(95% CI,1.054 - 1.368),P = 0.0056。接受多西他赛化疗的患者中,仅肠型患者的OS有所提高:HR为0.65(95% CI,0.49 - 0.87),P = 0.024,而有弥漫性成分的亚组患者OS无增加。关于无进展生存期(PFS),含多西他赛化疗方案的效果存在显著交互作用,与任何其他方案相比,仅肠型亚组的PFS更好:HR为0.65(95% CI,0.50 - 0.85),P = 0.015,与基于蒽环类药物的方案相比:HR为0.64(95% CI,0.46 - 0.88),P = 0.046。
总之,在本登记数据库中,劳伦分类的肿瘤亚型可预测生存期且对化疗的反应不同。未来的临床试验应根据组织学分层评估疗效。