Sato Junya, Mori Megumi, Nihei Satoru, Takeuchi Satoshi, Kashiwaba Masahiro, Kudo Kenzo
Department of Hospital Pharmacy, Iwate Medical University, 19-1 Uchimaru, Morioka, Iwate, 020-8505 Japan.
Department of Clinical Pharmaceutics, School of Pharmacy, 2-1-1 Nishitokuta, Yahaba, Iwate 028-3694 Japan.
J Pharm Health Care Sci. 2017 Jul 25;3:21. doi: 10.1186/s40780-017-0089-4. eCollection 2017.
In an evaluation of chemotherapy-induced peripheral neuropathy (CIPN), objectivity may be poor because the evaluation is determined by the patient's subjective assessment. In such cases, management of neuropathy may be delayed and CIPN symptoms may become severe. In this pilot study, we attempted an objective evaluation of CIPN using a quantitative pain measurement system (Pain Vision).
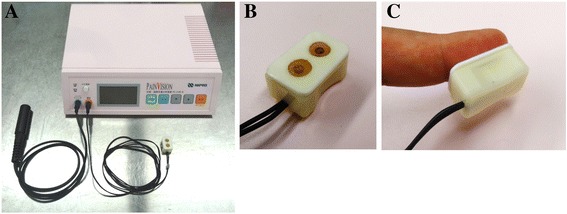
The subjects were patients with gynecologic cancer who underwent chemotherapy using taxane and platinum drugs. The grade of the peripheral sensory nerve disorder was based on the Common Terminology Criteria for Adverse Events (CTC-AE) ver. 4.0 and was evaluated before the initiation of therapy and up to six chemotherapy cycles. A symptom scale assessed by the patients using a peripheral neuropathy questionnaire (PNQ) was also evaluated. Simultaneously during these evaluations, graded electric current was applied from the probe to a fingertip and measured both the lowest perceptible current and lowest current perceived as pain by Pain Vision. From these values, the pain degree was calculated from the following formula: (pain perception current value - lowest perceptible current value) ÷ lowest perceptible current value × 100. We compared the pain degrees by Pain Vision during CIPN development with the value obtained before chemotherapy initiation.
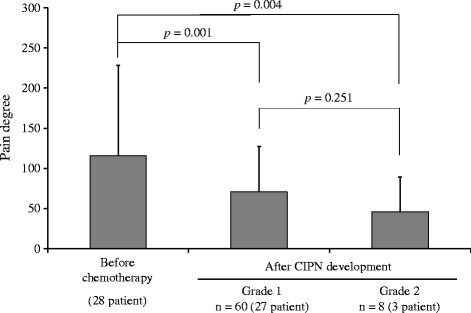
Forty-one patients were enrolled. In the evaluation by a medical professional, 28 (64.3%) patients developed CIPN during 2.5 ± 1.1 chemotherapy cycles (mean ± standard deviation). The pain degree by Pain Vision at grade 1 and 2 CIPN development according to the evaluation (CTC-AE) was significantly decreased compared to that before chemotherapy initiation (126.0 ± 114.5 vs. 69.8 ± 46.8, = 0.001, and 126.0 ± 114.5 vs. 32.8 ± 32.6, = 0.004). Changes in the pain degree by Pain Vision were also found during scale B and C, D CIPN development in the patient evaluation (PNQ) (115.9 ± 112.4 vs. 70.6 ± 56.5, = 0.005, and 115.9 ± 112.4 vs. 46.3 ± 42.9, = 0.004). In the 13 patients in whom CIPN did not occur, no significant decrease in the pain degree by Pain Vision was detected ( = 0.764). There was no discontinuation of the measurements because of adverse events such as discomfort from the electric current.
The decrease in the pain degree measured by Pain Vision was associated with the onset of CIPN symptoms. Particularly, detection of CIPN by Pain Vision was possible, though most of the CIPN that occurred was low grade or mild symptom. Pain Vision might become a noninvasive and convenient objective CIPN detection tool to supplement subjective CIPN evaluation.
The study approval number in the institution; H25-140. Registered December 17, 2013.
在化疗引起的周围神经病变(CIPN)评估中,客观性可能较差,因为评估取决于患者的主观评价。在这种情况下,神经病变的管理可能会延迟,CIPN症状可能会加重。在这项初步研究中,我们尝试使用定量疼痛测量系统(Pain Vision)对CIPN进行客观评估。
研究对象为接受紫杉烷和铂类药物化疗的妇科癌症患者。外周感觉神经障碍的分级基于《不良事件通用术语标准》(CTC-AE)第4.0版,在治疗开始前及最多六个化疗周期进行评估。还评估了患者使用外周神经病变问卷(PNQ)评估的症状量表。在这些评估的同时,将分级电流从探头施加到指尖,并通过Pain Vision测量最低可感知电流和最低被感知为疼痛的电流。根据这些值,通过以下公式计算疼痛程度:(疼痛感知电流值 - 最低可感知电流值)÷最低可感知电流值×100。我们将CIPN发生期间通过Pain Vision测量的疼痛程度与化疗开始前获得的值进行比较。
共纳入41例患者。在医学专业人员的评估中,28例(64.3%)患者在2.5±1.1个化疗周期(平均值±标准差)期间发生了CIPN。根据评估(CTC-AE),在1级和2级CIPN发生时,通过Pain Vision测量的疼痛程度与化疗开始前相比显著降低(126.0±114.5对69.8±46.8,P = 0.001;126.0±114.5对32.8±32.6,P = 0.004)。在患者评估(PNQ)的B级和C级、D级CIPN发生期间,也发现了通过Pain Vision测量的疼痛程度的变化(115.9±112.4对70.6±56.5,P = 0.005;115.9±112.4对46.3±42.9,P = 0.004)。在未发生CIPN的13例患者中,未检测到通过Pain Vision测量的疼痛程度有显著降低(P = 0.764)。未因电流不适等不良事件而中断测量。
Pain Vision测量的疼痛程度降低与CIPN症状的出现相关。特别是,尽管发生的大多数CIPN为低级别或轻度症状,但通过Pain Vision检测CIPN是可能的。Pain Vision可能成为一种无创且方便的客观CIPN检测工具,以补充主观的CIPN评估。
该机构的研究批准号;H25 - 140。于2013年12月17日注册。