Myer Landon, Iyun Victoria, Zerbe Allison, Phillips Tamsin K, Brittain Kirsty, Mukonda Elton, Allerton Joanna, Kalombo Cathy D, Nofemela Andile, Abrams Elaine J
Centre for Infectious Diseases Epidemiology & Research, School of Public Health & Family Medicine, University of Cape Town, Cape Town, South Africa.
Division of Epidemiology & Biostatistics, School of Public Health & Family Medicine, University of Cape Town, Cape Town, South Africa.
J Int AIDS Soc. 2017 Jul 21;20(Suppl 4):21636. doi: 10.7448/IAS.20.5.21636.
The numbers of women initiating lifelong antiretroviral therapy (ART) during pregnancy and postpartum is increasing rapidly, presenting a burden on health systems and an urgent need for scalable models of care for this population. In a pilot project, we referred postpartum women who initiated ART during pregnancy to a community-based model of differentiated ART services.
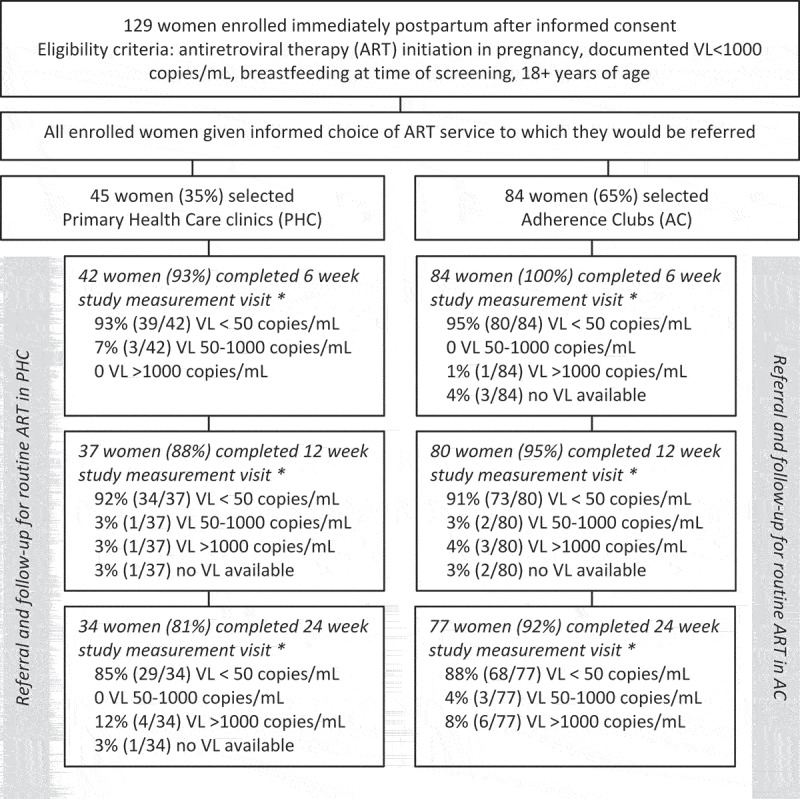
Eligible women (on ART for at least 3 months with viral load (VL)<1000 copies/mL) were offered a choice of two ART models of care: (i) referral to an existing system of community-based 'adherence clubs', operated by lay counsellors with medication collection every 2-4 months; or (ii) referral to local primary healthcare clinics (PHC) with services provided by clinicians and medication collection every 1-2 months (local standard of care for postpartum ART). For evaluation, women were followed through 6-months postpartum with VL testing separate from either ART service.
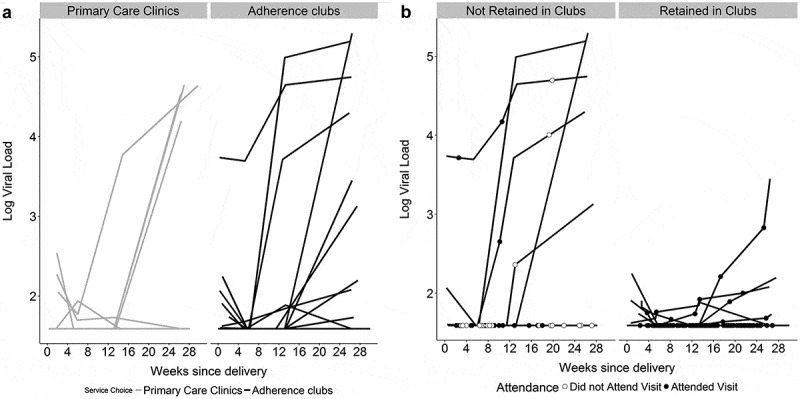
Through September 2015, = 129 women were enrolled (median age, 28 years; median time postpartum, 10 days). Overall, 65% ( = 84) chose adherence clubs and 35% ( = 45) chose PHCs; there were no demographic or clinical predictors of this choice. Location of service delivery was commonly cited as a reason for choice by women selecting either model of care; shorter waiting times, ability to receive ART from lay counsellors and less frequent appointments were motivations for choosing adherence clubs. Among women choosing adherence clubs, 15% never attended the service and another 11% attended the service but were not retained through six months postpartum. Overall, 86% of women ( = 111) remained in the evaluation through 6 months postpartum; in this group, there were no differences in VL<1000 copies/mL at six months postpartum between women choosing PHCs (88%) vs. adherence clubs (92%; = 0.483), but women who were not retained in adherence clubs were more likely to have VL≥1000 copies/mL compared to those who remained ( = 0.002).
Adherence clubs may be a valuable model for postpartum women initiating ART in pregnancy, with good short-term outcomes observed during this critical period. To support optimal implementation, further research is needed into patient preferences for models of care, with consideration of integration of maternal and child health services, while ART adherence and retention require ongoing consideration in this population.
孕期及产后开始接受终身抗逆转录病毒疗法(ART)的女性人数正在迅速增加,这给卫生系统带来了负担,并且迫切需要为这一人群提供可扩展的护理模式。在一个试点项目中,我们将孕期开始接受ART的产后女性转介至基于社区的差异化ART服务模式。
符合条件的女性(接受ART至少3个月且病毒载量(VL)<1000拷贝/毫升)可选择两种ART护理模式:(i)转介至现有的由非专业咨询师运营的社区“依从性俱乐部”系统,每2 - 4个月进行一次药物收集;或(ii)转介至当地基层医疗诊所(PHC),由临床医生提供服务,每1 - 2个月进行一次药物收集(产后ART的当地护理标准)。为进行评估,对女性进行产后6个月的随访,VL检测与任何一种ART服务分开进行。
截至2015年9月,共招募了129名女性(中位年龄28岁;中位产后时间10天)。总体而言,65%(n = 84)选择了依从性俱乐部,35%(n = 45)选择了PHC;没有人口统计学或临床因素可预测这一选择。服务提供地点是选择任何一种护理模式的女性常提到的选择原因;等待时间更短、能够从非专业咨询师处接受ART以及预约次数更少是选择依从性俱乐部的动机。在选择依从性俱乐部的女性中,15%从未参加过该服务,另有11%参加了该服务但在产后6个月内未持续接受服务。总体而言,86%的女性(n = 111)在产后6个月仍处于评估中;在这一组中,选择PHC的女性(88%)与选择依从性俱乐部的女性(92%;P = 0.483)在产后6个月时VL<1000拷贝/毫升方面没有差异,但与仍在接受服务的女性相比,未持续接受依从性俱乐部服务的女性更有可能VL≥1000拷贝/毫升(P = 0.002)。
依从性俱乐部可能是孕期开始接受ART的产后女性的一种有价值的模式,在这一关键时期观察到了良好的短期结果。为支持最佳实施,需要进一步研究患者对护理模式的偏好,同时考虑整合母婴健康服务,而对于这一人群,ART依从性和持续性仍需持续关注。