Fischer Janina, Pohl Alexandra, Volland Ruth, Hero Barbara, Dübbers Martin, Cernaianu Grigore, Berthold Frank, von Schweinitz Dietrich, Simon Thorsten
Department of Pediatric Oncology and Hematology, University Children's Hospital of Cologne, Kerpener Str. 62, 50924, Cologne, Germany.
Department of Pediatric Surgery, Dr. von Haunersches Children's Hospital, Munich, Germany.
BMC Cancer. 2017 Aug 4;17(1):520. doi: 10.1186/s12885-017-3493-0.
Although several studies have been conducted on the role of surgery in localized neuroblastoma, the impact of surgical timing and extent of primary tumor resection on outcome in high-risk patients remains controversial.
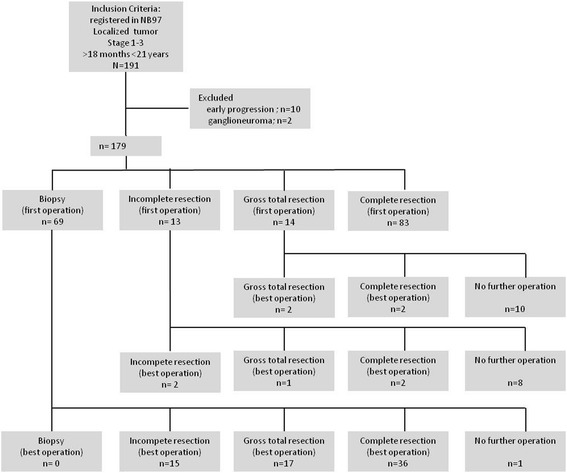
Patients from the German neuroblastoma trial NB97 with localized neuroblastoma INSS stage 1-3 age > 18 months were included for retrospective analysis. Imaging reports were reviewed by two independent physicians for Image Defined Risk Factors (IDRF). Operation notes and corresponding imaging reports were analyzed for surgical radicality. The extent of tumor resection was classified as complete resection (95-100%), gross total resection (90-95%), incomplete resection (50-90%), and biopsy (<50%) and correlated with local control rate and outcome. Patients were stratified according to the International Neuroblastoma Risk Group (INRG) staging system. Survival curves were estimated according to the method of Kaplan and Meier and compared by the log-rank test.
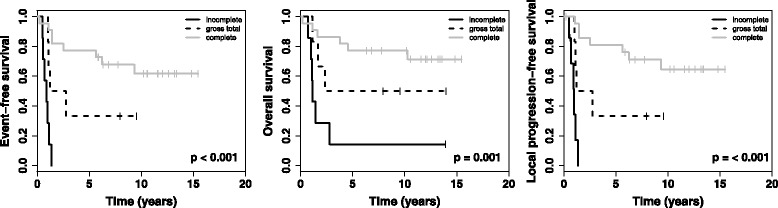
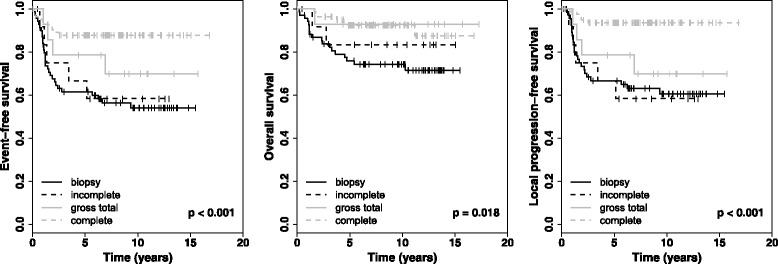
A total of 179 patients were included in this study. 77 patients underwent more than one primary tumor operation. After best surgery, 68.7% of patients achieved complete resection of the primary tumor, 16.8% gross total resection, 14.0% incomplete surgery, and 0.5% biopsy only. The cumulative complication rate was 20.3% and the surgery associated mortality rate was 1.1%. Image defined risk factors (IDRF) predicted the extent of resection. Patients with complete resection had a better local-progression-free survival (LPFS), event-free survival (EFS) and OS (overall survival) than the other groups. Subgroup analyses showed better EFS, LPFS and OS for patients with complete resection in INRG high-risk patients. Multivariable analyses revealed resection (complete vs. other), and MYCN (non-amplified vs. amplified) as independent prognostic factors for EFS, LPFS and OS.
In patients with localized neuroblastoma age 18 months or older, especially in INRG high-risk patients harboring MYCN amplification, extended surgery of the primary tumor site improved local control rate and survival with an acceptable risk of complications.
尽管已经有多项关于手术在局限性神经母细胞瘤中作用的研究,但手术时机和原发肿瘤切除范围对高危患者预后的影响仍存在争议。
纳入德国神经母细胞瘤试验NB97中年龄>18个月、局限性神经母细胞瘤INSS分期为1-3期的患者进行回顾性分析。两名独立医生对影像报告进行评估以确定影像定义风险因素(IDRF)。对手术记录和相应的影像报告进行分析以评估手术根治性。肿瘤切除范围分为完整切除(95-100%)、大体全切(90-95%)、部分切除(50-90%)和活检(<50%),并与局部控制率和预后相关联。患者根据国际神经母细胞瘤风险组(INRG)分期系统进行分层。根据Kaplan-Meier方法估计生存曲线,并通过对数秩检验进行比较。
本研究共纳入179例患者。77例患者接受了不止一次原发肿瘤手术。在最佳手术后,68.7%的患者实现了原发肿瘤的完整切除,16.8%为大体全切,14.0%为部分切除,仅0.5%为活检。累积并发症发生率为20.3%,手术相关死亡率为1.1%。影像定义风险因素(IDRF)可预测切除范围。完整切除的患者比其他组具有更好的无局部进展生存期(LPFS)、无事件生存期(EFS)和总生存期(OS)。亚组分析显示,INRG高危患者中完整切除的患者具有更好的EFS、LPFS和OS。多变量分析显示,切除情况(完整切除与其他)和MYCN(非扩增与扩增)是EFS、LPFS和OS的独立预后因素。
在18个月及以上的局限性神经母细胞瘤患者中,尤其是在伴有MYCN扩增的INRG高危患者中,对原发肿瘤部位进行扩大手术可提高局部控制率和生存率,且并发症风险可接受。