Department of Oncology, University of Cambridge, Cambridge, UK.
Clinical Trials and Statistics Unit, The Institute of Cancer Research, London, UK.
Lancet. 2017 Sep 9;390(10099):1048-1060. doi: 10.1016/S0140-6736(17)31145-5. Epub 2017 Aug 2.
Local cancer relapse risk after breast conservation surgery followed by radiotherapy has fallen sharply in many countries, and is influenced by patient age and clinicopathological factors. We hypothesise that partial-breast radiotherapy restricted to the vicinity of the original tumour in women at lower than average risk of local relapse will improve the balance of beneficial versus adverse effects compared with whole-breast radiotherapy.
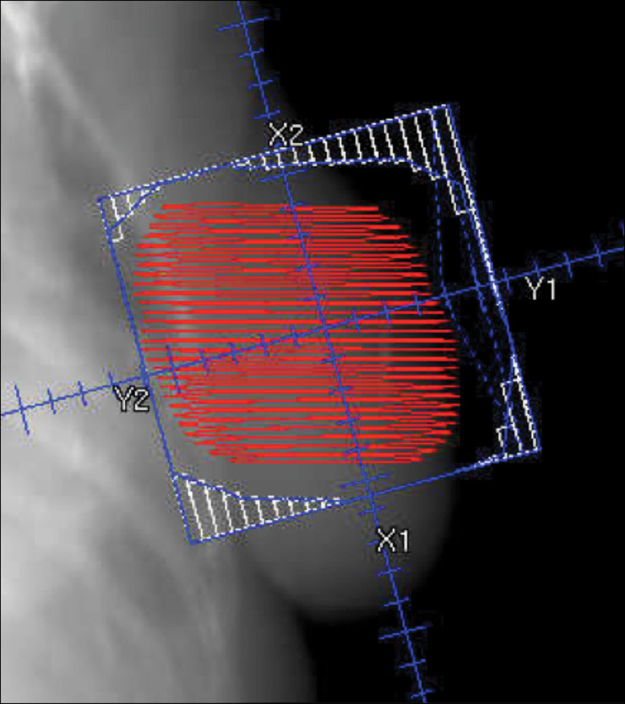
IMPORT LOW is a multicentre, randomised, controlled, phase 3, non-inferiority trial done in 30 radiotherapy centres in the UK. Women aged 50 years or older who had undergone breast-conserving surgery for unifocal invasive ductal adenocarcinoma of grade 1-3, with a tumour size of 3 cm or less (pT1-2), none to three positive axillary nodes (pN0-1), and minimum microscopic margins of non-cancerous tissue of 2 mm or more, were recruited. Patients were randomly assigned (1:1:1) to receive 40 Gy whole-breast radiotherapy (control), 36 Gy whole-breast radiotherapy and 40 Gy to the partial breast (reduced-dose group), or 40 Gy to the partial breast only (partial-breast group) in 15 daily treatment fractions. Computer-generated random permuted blocks (mixed sizes of six and nine) were used to assign patients to groups, stratifying patients by radiotherapy treatment centre. Patients and clinicians were not masked to treatment allocation. Field-in-field intensity-modulated radiotherapy was delivered using standard tangential beams that were simply reduced in length for the partial-breast group. The primary endpoint was ipsilateral local relapse (80% power to exclude a 2·5% increase [non-inferiority margin] at 5 years for each experimental group; non-inferiority was shown if the upper limit of the two-sided 95% CI for the local relapse hazard ratio [HR] was less than 2·03), analysed by intention to treat. Safety analyses were done in all patients for whom data was available (ie, a modified intention-to-treat population). This study is registered in the ISRCTN registry, number ISRCTN12852634.
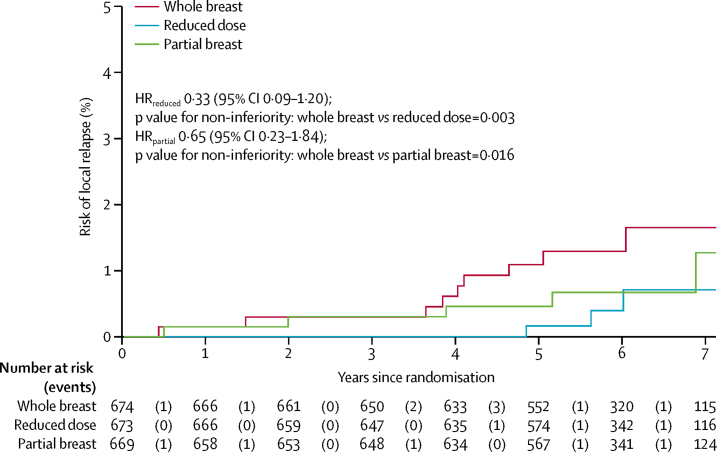
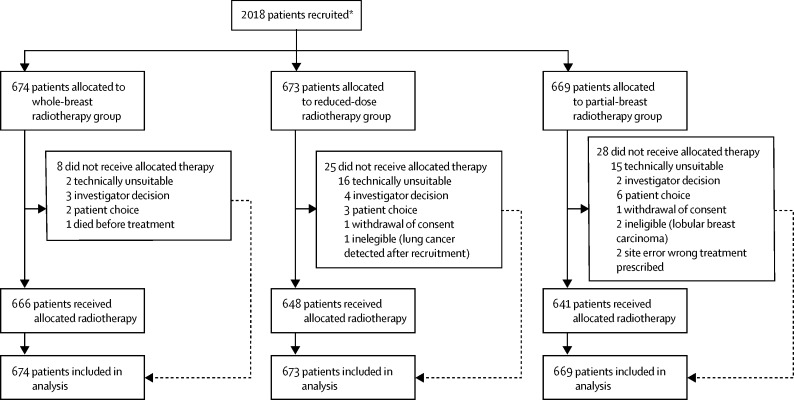
Between May 3, 2007, and Oct 5, 2010, 2018 women were recruited. Two women withdrew consent for use of their data in the analysis. 674 patients were analysed in the whole-breast radiotherapy (control) group, 673 in the reduced-dose group, and 669 in the partial-breast group. Median follow-up was 72·2 months (IQR 61·7-83·2), and 5-year estimates of local relapse cumulative incidence were 1·1% (95% CI 0·5-2·3) of patients in the control group, 0·2% (0·02-1·2) in the reduced-dose group, and 0·5% (0·2-1·4) in the partial-breast group. Estimated 5-year absolute differences in local relapse compared with the control group were -0·73% (-0·99 to 0·22) for the reduced-dose and -0·38% (-0·84 to 0·90) for the partial-breast groups. Non-inferiority can be claimed for both reduced-dose and partial-breast radiotherapy, and was confirmed by the test against the critical HR being more than 2·03 (p=0·003 for the reduced-dose group and p=0·016 for the partial-breast group, compared with the whole-breast radiotherapy group). Photographic, patient, and clinical assessments recorded similar adverse effects after reduced-dose or partial-breast radiotherapy, including two patient domains achieving statistically significantly lower adverse effects (change in breast appearance [p=0·007 for partial-breast] and breast harder or firmer [p=0·002 for reduced-dose and p<0·0001 for partial-breast]) compared with whole-breast radiotherapy.
We showed non-inferiority of partial-breast and reduced-dose radiotherapy compared with the standard whole-breast radiotherapy in terms of local relapse in a cohort of patients with early breast cancer, and equivalent or fewer late normal-tissue adverse effects were seen. This simple radiotherapy technique is implementable in radiotherapy centres worldwide.
Cancer Research UK.
在许多国家,接受保乳手术后联合放疗的乳腺癌局部复发风险已大幅下降,且该风险受患者年龄和临床病理因素影响。我们假设,在复发风险较低的女性中,将局部放疗限制在肿瘤原发病灶附近,而非全乳照射,与全乳放疗相比,其在有益效果和不良反应之间的平衡会更好。
IMPORT LOW 是一项在英国 30 个放疗中心进行的多中心、随机、对照、3 期非劣效性试验。纳入标准为:年龄 50 岁或以上,患有组织学分级为 1-3 级、肿瘤直径≤3cm(pT1-2)、腋窝淋巴结转移 0-3 个(pN0-1)、切缘有≥2mm 非癌组织的单侧浸润性导管腺癌,且接受保乳手术治疗。将患者按 1:1:1 随机分配接受全乳放疗 40Gy(对照组)、全乳放疗 36Gy 联合局部放疗 40Gy(减剂量组)或局部放疗 40Gy(部分乳房照射组),共 15 个分次。采用计算机生成的随机区组(大小为 6 和 9)进行分组,按放疗中心对患者进行分层。患者和临床医生对治疗分配不知情。采用标准切线野调强放疗,仅减少部分乳房照射组的照射野长度。主要终点为同侧局部复发(检验效能 80%,每组 5 年非劣效性界值为 2.5%;局部复发危险比[HR]的双侧 95%CI上限小于 2.03,则认为具有非劣效性),采用意向性治疗进行分析。对所有可评估数据的患者(即改良意向治疗人群)进行安全性分析。本研究在 ISRCTN 注册中心进行,编号 ISRCTN86626469。
2007 年 5 月 3 日至 2010 年 10 月 5 日期间共纳入 2018 名女性患者。其中 2 名患者撤回了数据分析同意。在全乳放疗(对照组)、减剂量组和部分乳房照射组中,分别有 674 例、673 例和 669 例患者可进行分析。中位随访时间为 72.2 个月(IQR 61.7-83.2),5 年局部复发累积发生率分别为对照组 1.1%(95%CI 0.5-2.3)、减剂量组 0.2%(0.02-1.2)和部分乳房照射组 0.5%(0.2-1.4)。与对照组相比,减剂量组和部分乳房照射组的 5 年绝对局部复发差异分别为-0.73%(-0.99 至 0.22)和-0.38%(-0.84 至 0.90)。减剂量组和部分乳房照射组的 HR 均大于 2.03,因此均能证明非劣效性(与全乳放疗组相比,p=0.003 和 p=0.016)。
在早期乳腺癌患者队列中,我们发现与标准全乳放疗相比,部分乳房和减剂量放疗在局部复发方面具有非劣效性,且迟发性正常组织不良反应更少或相当。这种简单的放疗技术在全球的放疗中心都可实施。
英国癌症研究中心。