GSK Clinical Unit Cambridge, Addenbrooke's Hospital NHS Trust, Cambridge, UK.
Clinical Pharmacology Modelling and Simulation Department, GSK, Stevenage, Herts, UK.
EBioMedicine. 2017 Aug;22:249-255. doi: 10.1016/j.ebiom.2017.07.020. Epub 2017 Jul 22.
The utility of intramuscular (IM) oxytocin for the prevention of postpartum hemorrhage in resource-poor settings is limited by the requirement for temperature-controlled storage and skilled staff to administer the injection. We evaluated the safety, tolerability and pharmacokinetics (PK) of a heat-stable, inhaled (IH) oxytocin formulation.
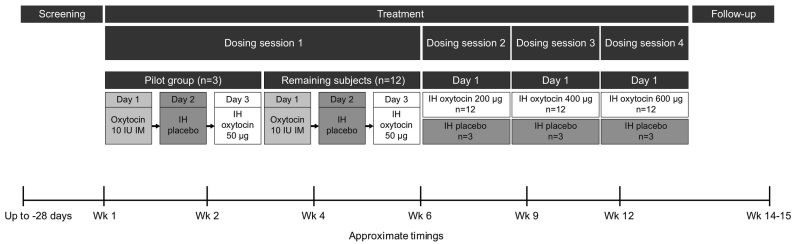
This phase 1, randomized, single-center, single-blind, dose-escalation, fixed-sequence study (NCT02542813) was conducted in healthy, premenopausal, non-pregnant, non-lactating women aged 18-45years. Subjects initially received IM oxytocin 10 international units (IU) on day 1, IH placebo on day 2, and IH oxytocin 50μg on day 3. Subjects were then randomized 4:1 using validated GSK internal software to IH placebo or ascending doses of IH oxytocin (200, 400, 600μg). PK was assessed by comparing systemic exposure (maximum observed plasma concentration, area under the concentration-time curve, and plasma concentrations at 10 and 30min post dose) for IH versus IM oxytocin. Adverse events (AEs), spirometry, laboratory tests, vital signs, electrocardiograms, physical examinations, and cardiac telemetry were assessed.
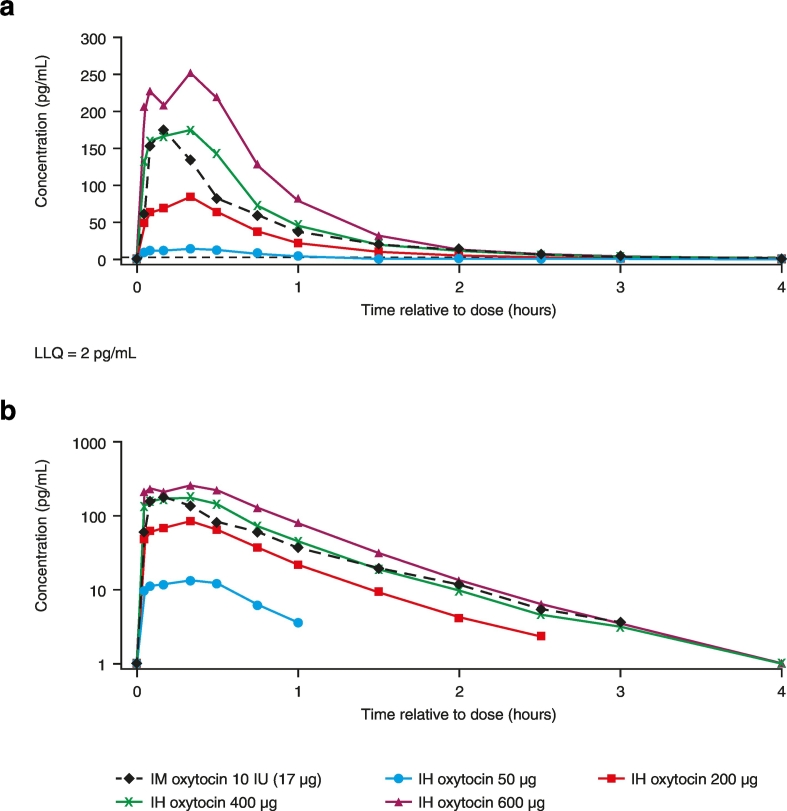
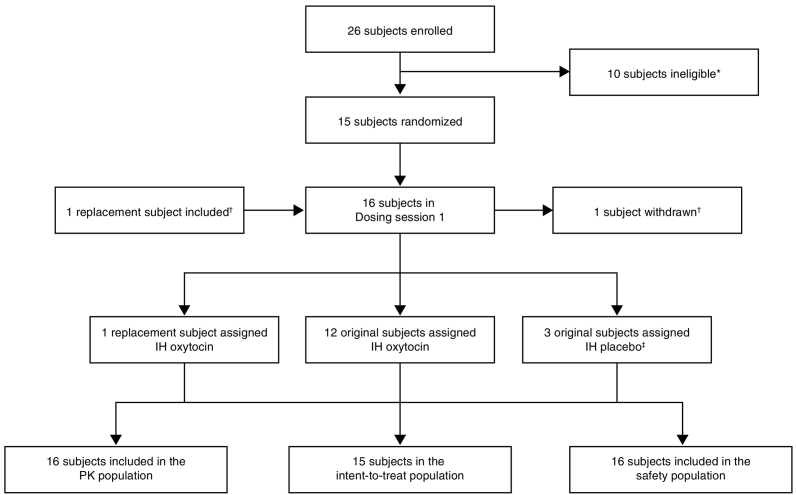
Subjects were recruited between September 14, 2015 and October 12, 2015. Of the 16 subjects randomized following initial dosing, 15 (IH placebo n=3; IH oxytocin n=12) completed the study. IH (all doses) and IM oxytocin PK profiles were comparable in shape. However, systemic exposure with IH oxytocin 400μg most closely matched IM oxytocin 10IU. Systemic exposure was approximately dose proportional for IH oxytocin. No serious AEs were reported. No clinically significant findings were observed for any safety parameters.
These data suggest that similar oxytocin systemic exposure can be achieved with IM and IH administration routes, and no safety concerns were identified with either route. The inhalation route may offer the opportunity to increase access to oxytocin for women giving birth in resource-poor settings.
在资源匮乏的环境中,肌肉内(IM)催产素用于预防产后出血的实用性受到限制,因为它需要温度控制储存和有技能的人员来注射。我们评估了一种热稳定、吸入(IH)催产素制剂的安全性、耐受性和药代动力学(PK)。
这是一项在健康、绝经前、非妊娠、非哺乳期 18-45 岁女性中进行的、随机、单中心、单盲、剂量递增、固定序列的 1 期研究(NCT02542813)。受试者最初在第 1 天接受 10 国际单位(IU)的 IM 催产素,第 2 天接受 IH 安慰剂,第 3 天接受 50μg 的 IH 催产素。然后,使用经过验证的 GSK 内部软件,根据 4:1 的比例将受试者随机分为 IH 安慰剂组或递增剂量的 IH 催产素组(200、400、600μg)。通过比较 IH 与 IM 催产素的系统暴露(最大观察到的血浆浓度、浓度-时间曲线下面积以及给药后 10 和 30 分钟的血浆浓度)来评估 PK。评估了不良事件(AE)、肺活量测定、实验室检查、生命体征、心电图、体格检查和心脏遥测。
受试者于 2015 年 9 月 14 日至 10 月 12 日期间被招募。在初始剂量后随机分组的 16 名受试者中,有 15 名(IH 安慰剂 n=3;IH 催产素 n=12)完成了研究。IH(所有剂量)和 IM 催产素 PK 曲线形状相似。然而,IH 催产素 400μg 的全身暴露与 IM 催产素 10IU 最为匹配。IH 催产素的全身暴露与剂量呈比例关系。未报告严重的 AE。任何安全性参数均未观察到临床显著发现。
这些数据表明,IM 和 IH 给药途径可实现相似的催产素全身暴露,且两种途径均未发现安全性问题。吸入途径可能为资源匮乏环境中分娩的妇女提供更多获得催产素的机会。