1 Division of Pediatric Neurology, Barrow Neurological Institute at Phoenix Children's Hospital , Phoenix, Arizona.
2 Department of Pediatric Neurology, Texas Children's Hospital , Baylor College of Medicine, Houston, Texas.
Brain Connect. 2017 Sep;7(7):424-442. doi: 10.1089/brain.2016.0479.
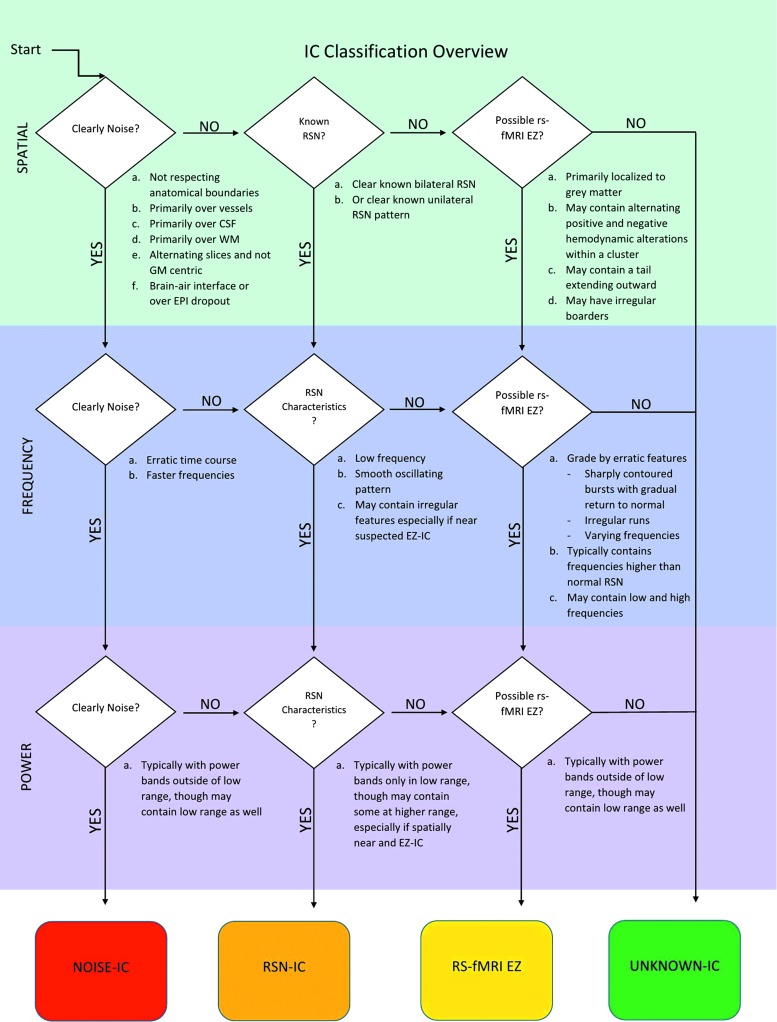
The purpose of this study was to prospectively investigate the agreement between the epileptogenic zone(s) (EZ) localization by resting-state functional magnetic resonance imaging (rs-fMRI) and the seizure onset zone(s) (SOZ) identified by intracranial electroencephalogram (ic-EEG) using novel differentiating and ranking criteria of rs-fMRI abnormal independent components (ICs) in a large consecutive heterogeneous pediatric intractable epilepsy population without an a priori alternate modality informing EZ localization or prior declaration of total SOZ number. The EZ determination criteria were developed by using independent component analysis (ICA) on rs-fMRI in an initial cohort of 350 pediatric patients evaluated for epilepsy surgery over a 3-year period. Subsequently, these rs-fMRI EZ criteria were applied prospectively to an evaluation cohort of 40 patients who underwent ic-EEG for SOZ identification. Thirty-seven of these patients had surgical resection/disconnection of the area believed to be the primary source of seizures. One-year seizure frequency rate was collected postoperatively. Among the total 40 patients evaluated, agreement between rs-fMRI EZ and ic-EEG SOZ was 90% (36/40; 95% confidence interval [CI], 0.76-0.97). Of the 37 patients who had surgical destruction of the area believed to be the primary source of seizures, 27 (73%) rs-fMRI EZ could be classified as true positives, 7 (18%) false positives, and 2 (5%) false negatives. Sensitivity of rs-fMRI EZ was 93% (95% CI 78-98%) with a positive predictive value of 79% (95% CI, 63-89%). In those with cryptogenic localization-related epilepsy, agreement between rs-fMRI EZ and ic-EEG SOZ was 89% (8/9; 95% CI, 0.52-99), with no statistically significant difference between the agreement in the cryptogenic and symptomatic localization-related epilepsy subgroups. Two children with negative ic-EEG had removal of the rs-fMRI EZ and were seizure free 1 year postoperatively. Of the 33 patients where at least 1 rs-fMRI EZ agreed with the ic-EEG SOZ, 24% had at least 1 additional rs-fMRI EZ outside the resection area. Of these patients with un-resected rs-fMRI EZ, 75% continued to have seizures 1 year later. Conversely, among 75% of patients in whom rs-fMRI agreed with ic-EEG SOZ and had no anatomically separate rs-fMRI EZ, only 24% continued to have seizures 1 year later. This relationship between extraneous rs-fMRI EZ and seizure outcome was statistically significant (p = 0.01). rs-fMRI EZ surgical destruction showed significant association with postoperative seizure outcome. The pediatric population with intractable epilepsy studied prospectively provides evidence for use of resting-state ICA ranking criteria, to identify rs-fMRI EZ, as developed by the lead author (V.L.B.). This is a high yield test in this population, because no seizure nor particular interictal epilepiform activity needs to occur during the study. Thus, rs-fMRI EZ detected by this technique are potentially informative for epilepsy surgery evaluation and planning in this population. Independent of other brain function testing modalities, such as simultaneous EEG-fMRI or electrical source imaging, contextual ranking of abnormal ICs of rs-fMRI localized EZs correlated with the gold standard of SOZ localization, ic-EEG, across the broad range of pediatric epilepsy surgery candidates, including those with cryptogenic epilepsy.
本研究的目的是前瞻性地调查在没有事先告知 EZ 定位的替代模式或预先宣布总 SOZ 数量的情况下,使用静息态功能磁共振成像(rs-fMRI)中异常独立成分(ICs)的新型区分和排序标准,与颅内脑电图(ic-EEG)确定的致痫区(EZ)之间的一致性。EZ 确定标准是通过对 350 名接受癫痫手术评估的儿科患者在 3 年内进行 rs-fMRI 的独立成分分析(ICA)来制定的。随后,这些 rs-fMRI EZ 标准被前瞻性地应用于 40 名接受 ic-EEG 以确定 SOZ 的评估队列。其中 37 名患者接受了认为是主要癫痫发作源的区域的手术切除/切断。术后收集了 1 年的癫痫发作频率。在评估的 40 名患者中,rs-fMRI EZ 与 ic-EEG SOZ 的一致性为 90%(36/40;95%置信区间[CI],0.76-0.97)。在接受认为是主要癫痫发作源的区域进行手术破坏的 37 名患者中,27 名(73%)rs-fMRI EZ 可被归类为真阳性,7 名(18%)为假阳性,2 名(5%)为假阴性。rs-fMRI EZ 的灵敏度为 93%(95%CI 78-98%),阳性预测值为 79%(95%CI,63-89%)。在与隐源性定位相关的癫痫患者中,rs-fMRI EZ 与 ic-EEG SOZ 的一致性为 89%(8/9;95%CI,0.52-99),隐源性和症状性定位相关癫痫亚组之间的一致性没有统计学意义。两名 ic-EEG 阴性的儿童切除了 rs-fMRI EZ,术后 1 年无癫痫发作。在至少有 1 个 rs-fMRI EZ 与 ic-EEG SOZ 一致的 33 名患者中,24%的患者在切除区域外至少有 1 个额外的 rs-fMRI EZ。在这些有未切除的 rs-fMRI EZ 的患者中,75%的患者在 1 年后仍有癫痫发作。相反,在 75%的 rs-fMRI 与 ic-EEG SOZ 一致且没有解剖上分离的 rs-fMRI EZ 的患者中,只有 24%的患者在 1 年后仍有癫痫发作。rs-fMRI EZ 与术后癫痫发作结果之间的这种关系具有统计学意义(p=0.01)。rs-fMRI EZ 的手术破坏与术后癫痫发作结果显著相关。本前瞻性研究的耐药性癫痫儿科患者提供了使用静息态 ICA 排序标准来识别 rs-fMRI EZ 的证据,该标准由主要作者(V.L.B.)开发。这是该人群中一种高收益的测试,因为在研究过程中不需要发生任何癫痫发作或特定的癫痫样活动。因此,通过该技术检测到的 rs-fMRI EZ 可能对该人群的癫痫手术评估和规划具有信息性。与其他脑功能测试模式(如同时进行 EEG-fMRI 或电源成像)无关,rs-fMRI 定位 EZ 的异常 IC 的独立上下文排序与 SOZ 定位的金标准 ic-EEG 相关,跨越了广泛的儿科癫痫手术候选人群,包括隐源性癫痫患者。