Hussain Shaun A, Mathern Gary W, Hung Phoebe, Weng Julius, Sankar Raman, Wu Joyce Y
Division of Pediatric Neurology, David Geffen School of Medicine and Mattel Children's Hospital UCLA,Los Angeles, CA, United States.
Departments of Neurosurgery and Psychiatry & Bio Behavioral Sciences, David Geffen School of Medicine, University of California, Los Angeles, CA United States; The Brain Research Institute, and The Intellectual and Developmental Disabilities Research Center, University of California, Los Angeles, United States.
Epilepsy Res. 2017 Sep;135:79-86. doi: 10.1016/j.eplepsyres.2017.06.010. Epub 2017 Jun 16.
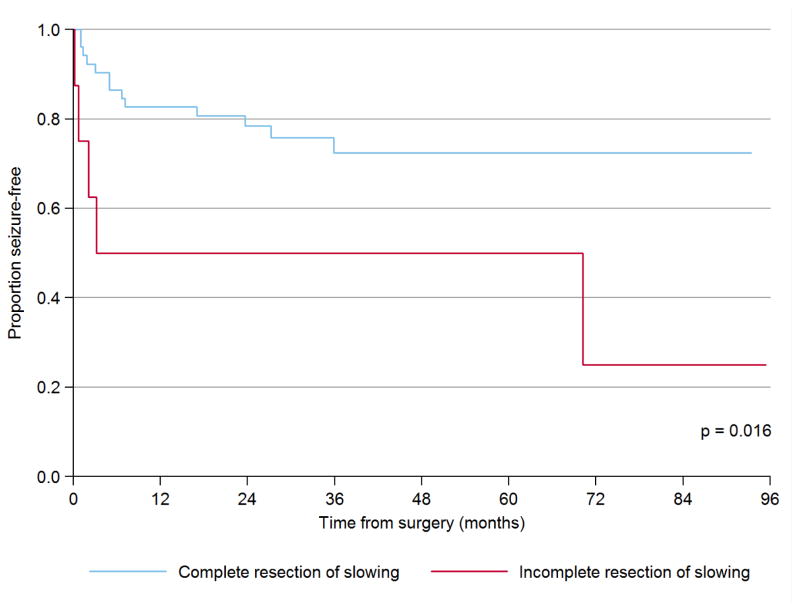
In the surgical management of epilepsy, the resection of cortex exhibiting interictal fast ripples (250-500Hz) on electrocorticography has been linked to postoperative seizure-freedom. Although fast ripples appear to accurately identify the epileptogenic zone-the minimum tissue that must be removed at surgery to achieve seizure-freedom-it has not been established that fast ripples are a superior biomarker in comparison with multimodal presurgical neuroimaging and other electrocorticography abnormalities. Hence, in the prediction of postoperative seizure-freedom, we compared the value of fast ripples with other intraoperative electocorticography abnormalities including focal slowing, paroxysmal fast activity, intermittent spike discharges, continuous epileptiform discharges, focal attenuation, and intraoperative seizures, as well as complete resection of the lesion defined by MRI and other neuroimaging. In a cohort of 60 children with lesional epilepsy and median postsurgical follow-up exceeding 4 years, who underwent resective epilepsy surgery with intraoperative electrocorticography, we evaluated the extent to which removal of each intraoperative electrocorticography abnormality impacts time to first postoperative seizure using the Kaplan-Meier method and Cox proportional hazards regression. Secondly, we contrasted the predictive value of resection of each competing electrocorticography abnormality using standard test metrics (sensitivity, specificity, positive predictive value, and negative predictive value). In contrast with all other intraoperative electrocorticography abnormalities, fast ripples demonstrated the most favorable combination of positive predictive value (100%) and negative predictive value (76%) in the prediction of postoperative seizures. Among all candidate electrocorticography features, time to first postoperative seizure was most strongly associated with incomplete resection of fast ripples (hazard ratio=19.8, p<0.001). In multivariate survival analyses, postoperative seizures were independently predicted by incomplete resection of cortex generating fast ripples (hazard ratio=25.4, 95%CI 6.71-96.0, p<0.001) and focal slowing (hazard ratio=5.79, 95%CI 1.76-19.0, p=0.004), even after adjustment for the impact of an otherwise complete resection. All children with incomplete resection of interictal FR-generating cortex exhibited postoperative seizures within six months. Notably, this cohort included many patients with large resections and thus limited opportunity to exhibit unresected fast ripples. Future study in a cohort with small resection volume, or a clinical trial in which resection margins are guided by fast ripple distribution, would likely yield a more precise estimate of the risk posed by unresected fast ripples. With a high detection rate during brief intraoperative electrocorticography and favorable positive and negative predictive value, interictal fast ripple characterization during surgery is a feasible and useful adjunct to standard methods for epilepsy surgery planning, and represents a valuable spatially-localizing biomarker of the epileptogenic zone, without the need for prolonged extraoperative electrocorticography.
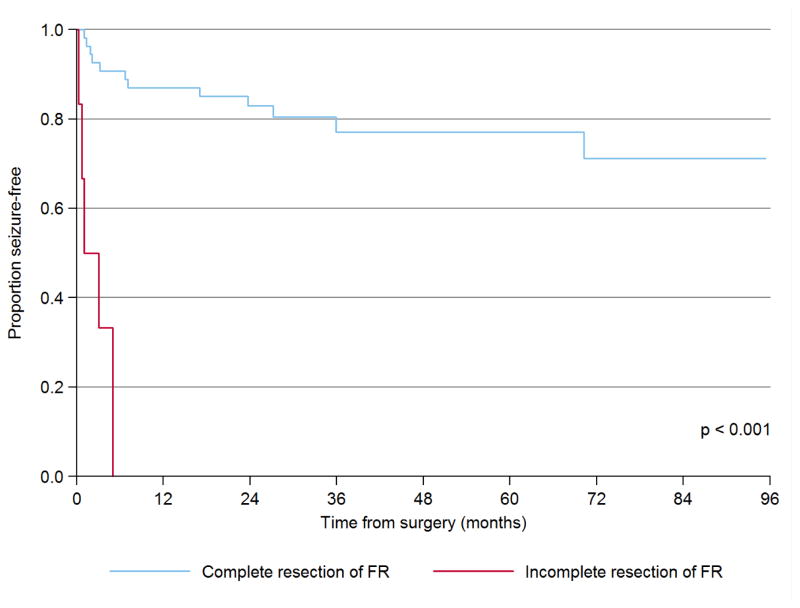
在癫痫的外科治疗中,切除皮质电图显示发作间期快波(250 - 500Hz)的皮质与术后无癫痫发作相关。尽管快波似乎能准确识别致痫区——手术中必须切除以实现无癫痫发作的最小组织——但与多模态术前神经影像学和其他皮质电图异常相比,尚未确定快波是一种更优的生物标志物。因此,在预测术后无癫痫发作方面,我们将快波的价值与其他术中皮质电图异常进行了比较,包括局灶性慢波、阵发性快活动、间歇性棘波放电、持续性癫痫样放电、局灶性衰减和术中癫痫发作,以及磁共振成像(MRI)和其他神经影像学所定义病变的完全切除。在一组60例患有病灶性癫痫且术后中位随访时间超过4年的儿童中,他们接受了术中皮质电图监测下的切除性癫痫手术,我们使用Kaplan - Meier方法和Cox比例风险回归评估了每种术中皮质电图异常的切除对首次术后癫痫发作时间的影响程度。其次,我们使用标准测试指标(敏感性、特异性、阳性预测值和阴性预测值)对比了每种竞争性皮质电图异常切除的预测价值。与所有其他术中皮质电图异常相比,快波在术后癫痫发作预测中显示出最有利的阳性预测值(100%)和阴性预测值(76%)组合。在所有候选皮质电图特征中,首次术后癫痫发作时间与快波未完全切除最密切相关(风险比 = 19.8,p < 0.001)。在多变量生存分析中,即使在调整了其他完全切除的影响后,术后癫痫发作仍可由产生快波的皮质未完全切除(风险比 = 25.4,95%置信区间6.71 - 96.0,p < 0.001)和局灶性慢波(风险比 = 5.79,95%置信区间1.76 - 19.0,p = 0.00)独立预测。所有发作间期产生快波的皮质未完全切除的儿童在6个月内均出现了术后癫痫发作。值得注意的是,该队列包括许多进行了大切除的患者,因此显示未切除快波的机会有限。未来在切除体积较小的队列中进行研究,或在一项以快波分布指导切除边缘的临床试验中,可能会更精确地估计未切除快波所带来的风险。由于在短暂的术中皮质电图监测期间检测率高,且具有良好的阳性和阴性预测值,手术期间发作间期快波特征是癫痫手术规划标准方法的一种可行且有用的辅助手段,并且代表了致痫区一种有价值的空间定位生物标志物,无需延长术外皮质电图监测时间。