Tørring M L, Murchie P, Hamilton W, Vedsted P, Esteva M, Lautrup M, Winget M, Rubin G
Department of Anthropology, School of Culture and Society, Aarhus University, Moesgaard Allé 20, Højbjerg DK-8270, Denmark.
Division of Applied Health Sciences, Centre of Academic Primary Care, University of Aberdeen, Polwarth Building, Foresterhill, Aberdeen AB25 2ZD, UK.
Br J Cancer. 2017 Sep 5;117(6):888-897. doi: 10.1038/bjc.2017.236. Epub 2017 Aug 8.
The benefits from expedited diagnosis of symptomatic cancer are uncertain. We aimed to analyse the relationship between stage of colorectal cancer (CRC) and the primary and specialist care components of the diagnostic interval.
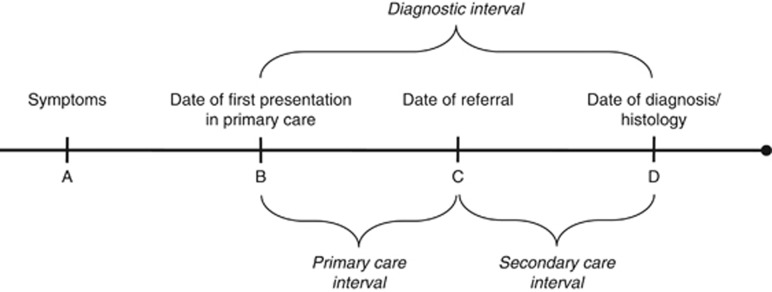
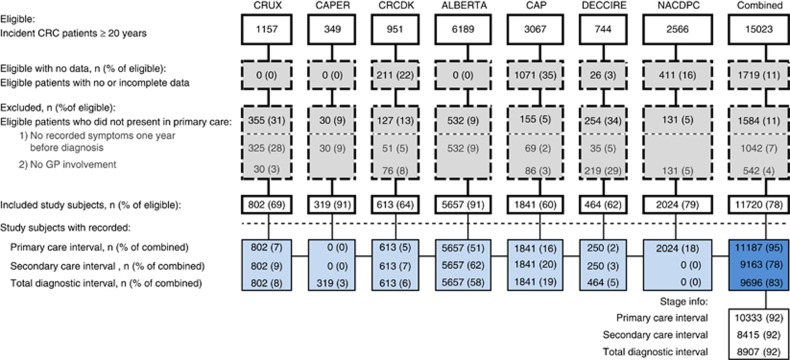
We identified seven independent data sets from population-based studies in Scotland, England, Canada, Denmark and Spain during 1997-2010 with a total of 11 720 newly diagnosed CRC patients, who had initially presented with symptoms to a primary care physician. Data were extracted from patient records, registries, audits and questionnaires, respectively. Data sets were required to hold information on dates in the diagnostic interval (defined as the time from the first presentation of symptoms in primary care until the date of diagnosis), symptoms at first presentation in primary care, route of referral, gender, age and histologically confirmed stage. We carried out reanalysis of all individual data sets and, using the same method, analysed a pooled individual patient data set.
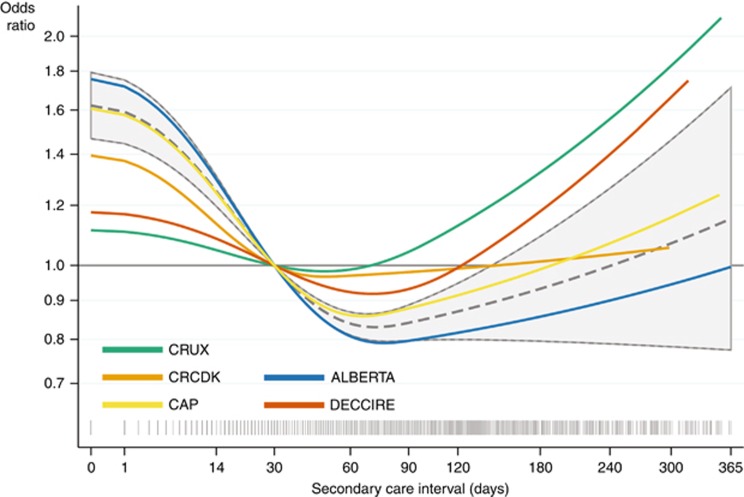
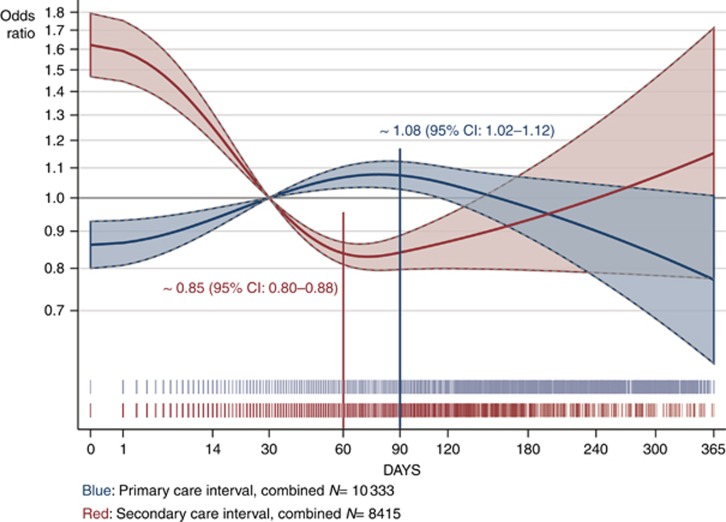
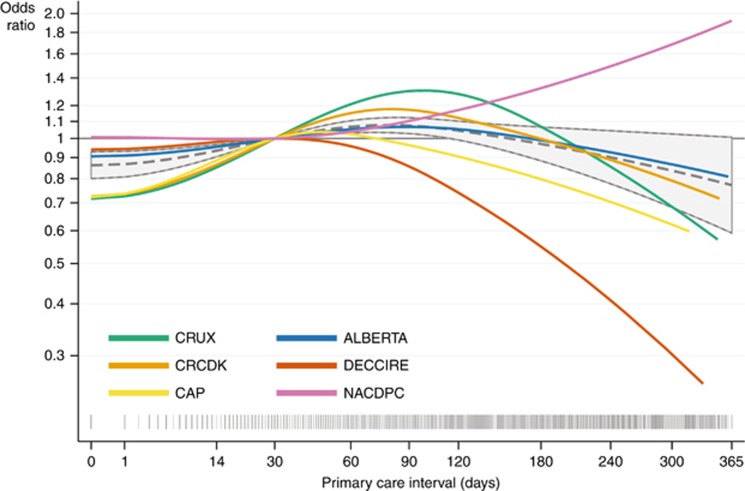
The association between intervals and stage was similar in the individual and combined data set. There was a statistically significant convex (∩-shaped) association between primary care interval and diagnosis of advanced (i.e., distant or regional) rather than localised CRC (P=0.004), with odds beginning to increase from the first day on and peaking at 90 days. For specialist care, we saw an opposite and statistically significant concave (∪-shaped) association, with a trough at 60 days, between the interval and diagnosis of advanced CRC (P<0.001).
This study provides evidence that longer diagnostic intervals are associated with more advanced CRC. Furthermore, the study cannot define a specific 'safe' waiting time as the length of the primary care interval appears to have negative impact from day one.
快速诊断有症状癌症的益处尚不确定。我们旨在分析结直肠癌(CRC)的分期与诊断间隔中的初级和专科护理组成部分之间的关系。
我们从1997年至2010年期间在苏格兰、英格兰、加拿大、丹麦和西班牙开展的基于人群的研究中识别出7个独立数据集,共有11720例新诊断的CRC患者,这些患者最初向初级保健医生报告了症状。数据分别从患者记录、登记处、审计和问卷中提取。要求数据集包含诊断间隔中的日期信息(定义为从初级保健中首次出现症状到诊断日期的时间)、初级保健中首次出现症状时的症状、转诊途径、性别、年龄以及组织学确诊的分期。我们对所有单个数据集进行了重新分析,并使用相同方法分析了一个汇总的个体患者数据集。
个体数据集和合并数据集中间隔与分期之间的关联相似。初级保健间隔与晚期(即远处或区域)而非局限性CRC的诊断之间存在统计学上显著的凸形(∩形)关联(P = 0.004),从第一天起比值开始增加,并在90天时达到峰值。对于专科护理,我们看到晚期CRC的诊断间隔与诊断之间存在相反且统计学上显著的凹形(∪形)关联,在60天时出现低谷(P < 0.001)。
本研究提供了证据表明更长的诊断间隔与更晚期的CRC相关。此外,由于初级保健间隔的时长似乎从第一天起就有负面影响,该研究无法确定一个特定 的“安全”等待时间。