Miyabe Junji, Hanamoto Atsushi, Tatsumi Mitsuaki, Hamasaki Toshimitsu, Takenaka Yukinori, Nakahara Susumu, Kishikawa Toshihiro, Suzuki Motoyuki, Takemoto Norihiko, Michiba Takahiro, Yoshioka Yasuo, Isohashi Fumiaki, Konishi Koji, Ogawa Kazuhiko, Hatazawa Jun, Inohara Hidenori
Department of Otorhinolaryngology-Head and Neck Surgery, Osaka University School of Medicine, Osaka, Japan.
Department of Nuclear Medicine and Tracer Kinetics, Osaka University Graduate School of Medicine, Osaka, Japan.
Cancer Sci. 2017 Oct;108(10):2030-2038. doi: 10.1111/cas.13345. Epub 2017 Aug 30.
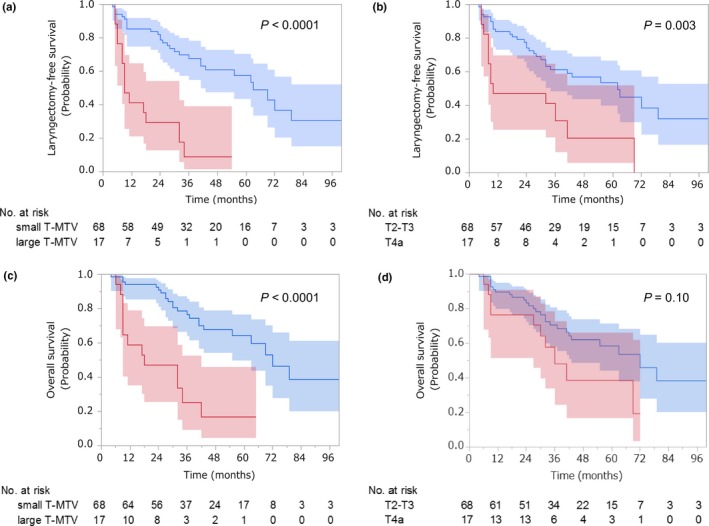
We aimed to determine whether pretreatment metabolic tumor volume of the primary tumor (T-MTV) or T classification would be a better predictor of laryngectomy-free survival (LFS) and overall survival (OS) after chemoradiotherapy in patients with locally advanced laryngeal or hypopharyngeal cancer requiring total laryngectomy. We analyzed 85 patients using a Cox proportional hazards model and evaluated its usefulness by Akaike's information criterion. A T-MTV cut-off value was determined by time-dependent receiver operating characteristic curve analysis. Interobserver reliability for measuring T-MTV was estimated by the intraclass correlation coefficient (ICC). After adjustment for covariables, T-MTV, irrespective of whether a continuous or dichotomized variable, and T classification remained independent predictors of LFS and OS. Large T-MTV (>28.7 mL) was associated with inferior LFS (hazard ratio [HR], 4.16; 95% confidence interval [CI], 1.97-8.70; P = 0.0003) and inferior OS (HR, 3.18; 95% CI, 1.47-6.69; P = 0.004) compared with small T-MTV (≤28.7 mL). The T-MTV model outperformed the T classification model in predicting LFS and OS (P = 0.007 and 0.01, respectively). Three-year LFS and OS rates for patients with small versus large T-MTV were 68% vs 9% (P < 0.0001) and 77% vs 25% (P < 0.0001), respectively, whereas those for patients with T2-T3 versus T4a were 61% vs 31% (P = 0.003) and 71% vs 48% (P = 0.10), respectively. ICC was 0.99 (95% CI, 0.99-1.00). Given the excellent interobserver reliability, T-MTV is better than T classification to identify patients who would benefit from the larynx preservation approach.
我们旨在确定,对于需要进行全喉切除术的局部晚期喉癌或下咽癌患者,原发肿瘤的预处理代谢肿瘤体积(T-MTV)或T分期,哪一个能更好地预测放化疗后的无喉生存率(LFS)和总生存率(OS)。我们使用Cox比例风险模型分析了85例患者,并通过赤池信息准则评估其有效性。通过时间依赖性受试者工作特征曲线分析确定T-MTV的临界值。通过组内相关系数(ICC)估计测量T-MTV的观察者间可靠性。在对协变量进行调整后,无论T-MTV是连续变量还是二分变量,以及T分期,仍然是LFS和OS的独立预测因素。与小T-MTV(≤28.7 mL)相比,大T-MTV(>28.7 mL)与较差的LFS(风险比[HR],4.16;95%置信区间[CI],1.97-8.70;P = 0.0003)和较差的OS(HR,3.18;95% CI,1.47-6.69;P = 0.004)相关。在预测LFS和OS方面,T-MTV模型优于T分期模型(分别为P = 0.007和0.01)。小T-MTV与大T-MTV患者的三年LFS率和OS率分别为68%对9%(P < 0.0001)和77%对25%(P < 0.0001),而T2-T3与T4a患者的三年LFS率和OS率分别为61%对31%(P = 0.003)和71%对48%(P = 0.10)。ICC为0.99(95% CI,0.99-1.00)。鉴于观察者间可靠性极佳,T-MTV在识别可从保喉方法中获益的患者方面优于T分期。