Bezuska Laurynas, Lebetkevicius Virgilijus, Sudikiene Rita, Liekiene Daina, Tarutis Virgilijus
Department of Cardiovascular Medicine, Vilnius University, Santariskiu 2, 08661, Vilnius, Lithuania.
Centre of Cardiac Surgery, Vilnius University Hospital Santariskiu Klinikos, Santariskiu 2, 08661, Vilnius, Lithuania.
J Cardiothorac Surg. 2017 Aug 9;12(1):67. doi: 10.1186/s13019-017-0634-0.
The Fontan procedure has been modified several times since it was introduced into practice in 1968. As many patients now survive to adulthood, attention is directed towards their clinical status and late morbidity. We report our surgical experience of 30 years in Fontan procedures.
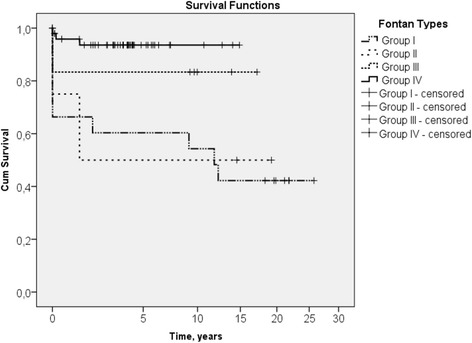
From January 1985 to January 2015, 80 patients underwent Fontan surgery. Twenty-one patients received an atrio-pulmonary Fontan (Group I), four patients underwent total cavopulmonary connection (TCPC) with an intra-atrial lateral tunnel (Group II), six patients received extra-cardiac TCPC with an aortic homograft (group III) and 49 patients received extra-cardiac TCPC with an expanded polytetrafluoroethylene conduit. They were followed for early and late mortality, long-term survival, postoperative morbidity and reoperations.
The mean follow-up time was 7.4 ± 6.6 years. The Kaplan-Meier estimated 15-year survival rate was 42% in Group I, 50% in Group II, 83% in Group III and 94% in Group IV. The median length of stay in intensive care unit, intubation and chest drain stay time were 90 h (IQR, 46-119), 8 h (IQR, 6-16) and 18 days (IQR, 12-28) respectively. Early complications were bleeding (6), taken down of Fontan circulation (3) and acute heart failure managed by left heart bypass (1). Late-occurring morbidities included arrhythmias (6), protein-losing enteropathy (2), thromboembolism (2) and tracheal stenosis (1). Fourteen patients (18%) had redo Fontan procedures.
Our series showed improving results after Fontan completion with excellent mid-term outcome after extra-cardiac TCPC with expanded polytetrafluoroethylene conduit. The long-term result should be followed.
自1968年应用于临床以来,Fontan手术已历经多次改良。由于现在许多患者存活至成年,因此关注焦点转向他们的临床状况和晚期发病率。我们报告我们30年的Fontan手术外科经验。
1985年1月至2015年1月,80例患者接受了Fontan手术。21例患者接受了心房-肺动脉Fontan手术(第一组),4例患者采用心房内侧面隧道进行全腔静脉-肺动脉连接(TCPC)(第二组),6例患者采用主动脉同种异体移植物进行心外TCPC(第三组),49例患者采用膨体聚四氟乙烯导管进行心外TCPC。对他们进行早期和晚期死亡率、长期生存率、术后发病率及再次手术情况的随访。
平均随访时间为7.4±6.6年。Kaplan-Meier法估计第一组15年生存率为42%,第二组为50%,第三组为83%,第四组为94%。重症监护病房的中位住院时间、插管时间和胸腔引流停留时间分别为90小时(四分位间距,46 - 119)、8小时(四分位间距,6 - 16)和18天(四分位间距,12 - 28)。早期并发症包括出血(6例)、Fontan循环拆除(3例)和通过左心旁路治疗的急性心力衰竭(1例)。晚期发病包括心律失常(6例)、蛋白丢失性肠病(2例)、血栓栓塞(2例)和气管狭窄(1例)。14例患者(18%)接受了再次Fontan手术。
我们的系列研究显示,Fontan手术完成后结果有所改善,采用膨体聚四氟乙烯导管进行心外TCPC后的中期结果良好。应持续关注长期结果。