Sandvig Axel, Lundberg Sandra, Neuwirth Jiri
Department of Pharmacology and Clinical Neurosciences, Division of Neuro, Head and Neck, Umeå University Hospital, Umeå, Sweden.
Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Trondheim, Norway.
J Med Case Rep. 2017 Aug 12;11(1):221. doi: 10.1186/s13256-017-1375-3.
The artery of Percheron is a rare anatomic variant of arterial supply to the paramedian thalamus and rostral midbrain, and occlusion of the artery of Percheron results in bilateral paramedian thalamic infarcts with or without midbrain involvement. Acute artery of Percheron infarcts represent 0.1 to 2% of total ischemic stroke. However, of thalamic strokes, occlusion of artery of Percheron is the cause in 4 to 35% of cases. Early diagnosis of artery of Percheron infarction can be challenging because it is infrequent and early computed tomography or magnetic resonance imaging may be negative. Thus, it can be confused with other neurological conditions such as tumors and infections.
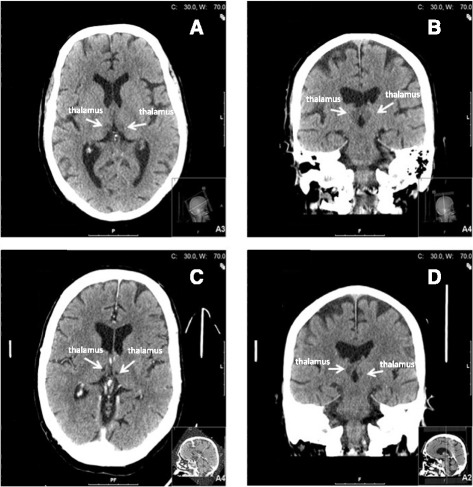
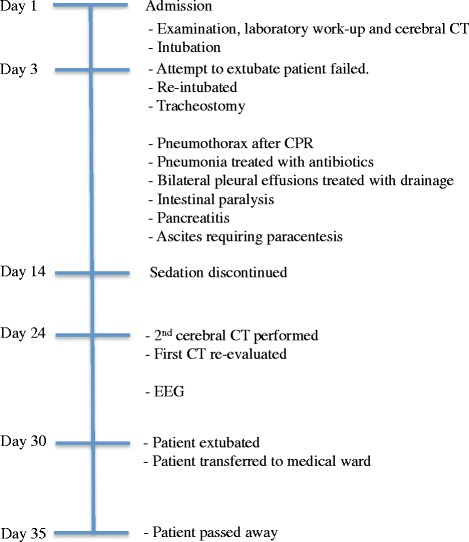
This is a retrospective case study of a 56-year-old white man admitted to Umeå University Hospital and diagnosed with an artery of Percheron infarction. Medical records and the neuroradiological database were reviewed, and the diagnosis was made based on typical symptoms and radiological findings of artery of Percheron infarction. We report the case of a 56-year-old man with a history of overconsumption of alcohol who was found in his home unconscious and hypothermic. He had a Reaction Level Scale-85 score of 4. He developed ventricular fibrillation on arrival at our emergency department, and cardiopulmonary resuscitation successfully restored sinus rhythm within an estimated 2 minutes of onset. He was then put on cardiopulmonary bypass for rewarming. The initial head computed tomography performed on admission was wrongly assessed as unremarkable. Bilateral ischemia in the paramedian thalamic nuclei and pons were first documented on a follow-up computed tomography on day 24 after hospitalization. He died on day 35 after hospitalization.
Artery of Percheron infarcts are rare. The radiological diagnosis can initially often be judged as normal and in combination with variability in the neurological symptoms it is a rather difficult condition to diagnose. For these reasons few clinicians have much experience with this type of infarct, which may delay diagnosis and initiation of appropriate treatment.
佩谢隆动脉是供应丘脑旁正中核和中脑嘴侧的一种罕见动脉解剖变异,佩谢隆动脉闭塞会导致双侧丘脑旁正中梗死,可伴有或不伴有中脑受累。急性佩谢隆动脉梗死占全部缺血性卒中的0.1%至2%。然而,在丘脑卒中病例中,佩谢隆动脉闭塞占4%至35%。佩谢隆动脉梗死的早期诊断具有挑战性,因为其发病率低,早期计算机断层扫描(CT)或磁共振成像(MRI)可能为阴性。因此,它可能与肿瘤和感染等其他神经系统疾病相混淆。
这是一项对一名56岁白人男性的回顾性病例研究,该患者入住于默奥大学医院并被诊断为佩谢隆动脉梗死。查阅了病历和神经放射学数据库,并根据佩谢隆动脉梗死的典型症状和放射学表现做出诊断。我们报告了一名有酗酒史的56岁男性病例,他在家中被发现意识不清且体温过低。他的反应水平量表-85评分为4分。到达我们急诊科时他发生了心室颤动,心肺复苏在发作后约2分钟内成功恢复窦性心律。然后他接受体外循环复温。入院时进行的首次头部CT被错误地评估为无异常。住院后第24天的随访CT首次记录了丘脑旁正中核和脑桥的双侧缺血。他在住院后第35天死亡。
佩谢隆动脉梗死很罕见。放射学诊断最初通常可判断为正常,并且由于神经症状的变异性,这是一种相当难以诊断的疾病。由于这些原因,很少有临床医生对这种类型的梗死有很多经验,这可能会延迟诊断和启动适当的治疗。